Abstract
Type 2 endoleak (T2EL) is the most common complication after endovascular aneurysm repair (EVAR), occurring in 10%–25% of patients. Although many T2ELs follow a benign course, persistent T2EL is associated with sac expansion, secondary endoleaks, rupture, and aneurysm-related mortality. Endovascular treatment is indicated in cases of progressive sac growth and is broadly divided into the transarterial approach and the direct sac puncture approach—the latter encompassing transabdominal, translumbar, and transcaval routes. Each approach has distinct technical advantages and limitations, and selection should be tailored to the source vessel of the endoleak, sac location, surrounding anatomy, and patient-related factors. Coils, N-butyl cyanoacrylate, and ethylene vinyl alcohol copolymer (Onyx) constitute the principal embolic agents, with liquid embolics showing improved durability over coils alone in recent comparative studies. Prophylactic embolization of the inferior mesenteric artery, lumbar arteries, or the aneurysm sac during EVAR has recently emerged as a promising preventive strategy. This review summarizes the current approaches, embolic materials, prophylactic strategies, and clinical outcomes of T2EL management from the perspective of the interventional radiologist.
-
Keywords: Aortic aneurysm, abdominal; Endoleak; Endovascular aneurysm repair; Embolization, therapeutic
Introduction
Type 2 endoleak (T2EL) is the most common complication after endovascular aneurysm repair (EVAR) for abdominal aortic aneurysm (AAA), occurring in approximately 10%–25% of patients [
1,
2]. T2EL results from retrograde flow into the aneurysm sac via patent aortic side branches, most commonly the inferior mesenteric artery (IMA) and lumbar arteries (LAs), and less frequently from accessory renal, median sacral, vasa vasorum, or intercostal arteries [
2,
3]. It typically behaves as a hemodynamic system with inflow and outflow vessels, analogous to an arteriovenous malformation nidus, which has important implications for treatment strategy [
4].
Although many T2ELs follow a benign course and resolve spontaneously, persistent T2EL may lead to sac expansion, secondary type I or III endoleaks, sac rupture, and the need for reintervention or open conversion [
5]. Recent evidence has challenged the long-held notion that T2EL is uniformly benign. Large-scale registries and systematic reviews have shown that persistent T2EL—particularly when it persists beyond 1 year—is significantly associated with sac enlargement, reintervention, rupture, and AAA-related mortality after EVAR, and that active management is warranted in patients with progressive sac growth [
6-
8].
Current treatment guidelines have been updated to reflect this evolving evidence. The Society for Vascular Surgery recommends intervention when aneurysm sac expansion is ≥5 mm, whereas the updated European Society for Vascular Surgery (ESVS) guidelines use a sac growth threshold of >10 mm and provide revised recommendations on the diagnostic step-up and management of endoleaks, including a strengthened role for active management in high-risk patients with persistent T2EL [
9,
10].
This review provides a comprehensive update on the endovascular management of T2EL from the interventional radiologist's perspective, focusing on (1) approach techniques, (2) embolic materials, (3) prophylactic embolization, and (4) clinical outcomes.
Approach Techniques
Endovascular access routes for T2EL embolization are broadly divided into the transarterial approach (TAA) and the direct sac puncture approach. Alternative and emerging techniques are presented at the end of this section. A comparative summary is provided in
Table 1.
The TAA is one of the most commonly used techniques for T2EL embolization. Access is typically obtained from a femoral or brachial route, and catheterization of the endoleak is performed via collateral pathways depending on the source vessel. For IMA-driven endoleaks, the most common route is via the SMA through the marginal artery of Drummond or the arc of Riolan into the IMA, and subsequently into the endoleak nidus (
Fig. 1). For LA-driven endoleaks, the internal iliac artery and its iliolumbar collateral branches serve as the principal access route (
Fig. 2).
To minimize the risk of recurrence, both the feeding vessel and the endoleak nidus should be embolized. Embolization of the feeder alone is associated with high recurrence rates due to recruitment of additional collateral vessels [
4,
11]. Recent advances such as triaxial microcatheter systems and small-caliber microcatheters have improved the technical feasibility of navigating long and tortuous collateral pathways [
12].
Advantages of TAA include supine patient positioning, familiarity to the interventional radiologist, the minimally invasive nature of the procedure, and the ability to address multiple feeding vessels in a single session. However, this approach carries important technical limitations. In particular, LA-driven endoleaks require navigation through the iliolumbar collateral pathway from the internal iliac artery, which is frequently tortuous, narrow-caliber, and prone to spasm. As a result, super-selective access to the endoleak nidus through this circuitous route is technically demanding and often unsuccessful. Even when the feeding vessel is reached, definitive nidus embolization may be limited by the inability to advance the microcatheter sufficiently into the sac. These anatomic and technical considerations make TAA particularly suitable for IMA-dominant endoleaks with a favorable SMA-IMA collateral, whereas alternative direct sac puncture approaches are frequently required for LA-dominant endoleaks.
Direct Sac Puncture Approach
Direct sac puncture approaches involve percutaneous access into the aneurysm sac, allowing direct catheterization and embolization of the endoleak nidus and outflow vessels. These techniques are generally associated with higher technical success rates than the TAA, particularly for complex or multi-source endoleaks [
13]. Three principal routes have been described—transabdominal, translumbar, and transcaval—each chosen based on sac location, surrounding anatomy, and patient positioning constraints.
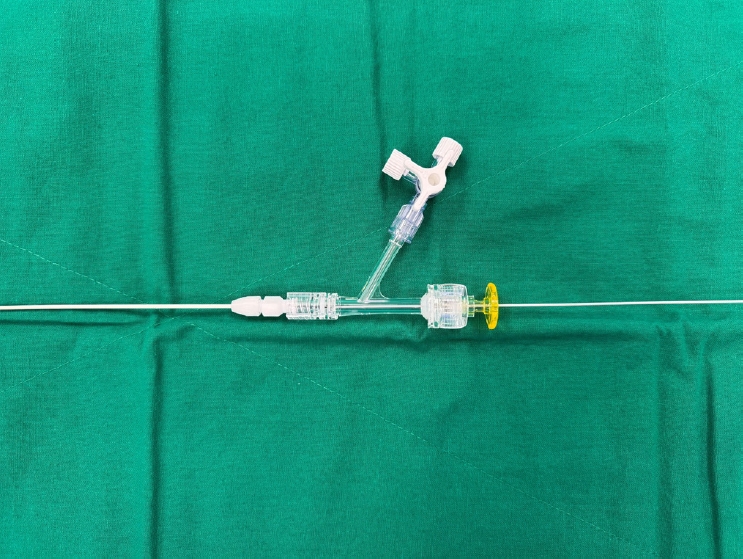
The technical workflow for both transabdominal and translumbar approaches follows a common sequence. Under CT, fluoroscopy, or ultrasound guidance, the endoleak nidus is punctured with a 21-gauge Chiba needle, and intrasac position is confirmed by free backflow of arterial blood. Selective angiography is then performed to delineate the endoleak nidus, feeding artery, and outflow vessels. A 0.018-inch guidewire is then introduced, and a 4-Fr coaxial introducer sheath is placed. A Y-connector is attached to the sheath to permit coaxial introduction of a microcatheter (
Fig. 3). In selected cases with low-flow dynamics and simple sac anatomy—particularly endoleaks supplied by a small number (typically 1–2) of feeders arising from a single vertebral level—the liquid embolic agent may also be injected directly through the 21-gauge Chiba puncture needle without subsequent placement of a coaxial introducer sheath and microcatheter [
14].
When the feeding artery can be selectively catheterized with the microcatheter, coil embolization is performed for feeder occlusion followed by a liquid embolic agent for nidus filling (
Fig. 4). When selective feeder catheterization is not possible, a liquid embolic alone is used to obliterate both the nidus and the proximal portion of the feeding artery.
The direct transabdominal approach involves anterior percutaneous puncture of the aneurysm sac under CT or ultrasound guidance, typically with the patient in the supine position. This approach is most suitable when the aneurysm sac has an accessible anterior window, free of overlying bowel, kidney, or vascular structures. While the supine positioning is well tolerated, careful pre-procedural planning with cross-sectional imaging is essential to avoid injury to adjacent abdominal organs [
15]. Disadvantages of the transabdominal approach include the risk of injury to overlying abdominal organs and limited applicability when no safe anterior puncture window is available.
The translumbar approach (TLA) is the most established direct sac puncture technique. With the patient in the prone position, percutaneous puncture is performed via a left posterolateral route under CT or CBCT guidance, and embolization is carried out under fluoroscopy. TLA provides excellent direct access to the sac and is particularly useful for LA-driven endoleaks. Disadvantages include the requirement for prone positioning—which may be challenging in elderly or obese patients—the risk of retroperitoneal hematoma, and limited applicability when bowel, kidney, or graft components are interposed in the puncture trajectory [
16-
18].
Transcaval embolization (TCE) is performed via transfemoral or transjugular venous access, with direct puncture of the IVC into the aneurysm sac. The level of the endoleak nidus is identified on pre-procedural CT angiography. Under fluoroscopic and intravascular ultrasound (IVUS) guidance, the Colapinto needle or the Rösch-Uchida needle is advanced from the IVC into the aneurysm sac at the planned level. After confirmation of intrasac position by angiography, embolization is typically performed using a liquid embolic agent to fill the endoleak nidus and outflow vessels [
19,
20]. Ideal candidates have a sac abutting the IVC with minimal calcification at the puncture site. The transcaval approach is particularly valuable when the endoleak nidus is located in a region inaccessible to transabdominal or translumbar approaches (
Fig. 5). Advantages of TCE include supine positioning, concurrent arterial access for completion angiography, and avoidance of risks associated with prone positioning, making it particularly valuable when transarterial and translumbar approaches have failed or are not feasible [
20,
21]. However, the main limitations are the risk of endograft injury and the technical complexity of caval-aortic crossing, although novel microwire-based caval traversal techniques have improved procedural safety [
22].
Several alternative and emerging approaches have been described for selected cases or as salvage strategies when conventional techniques fail. The perigraft approach involves catheterization of the space between the stent graft and the native aortic wall, typically via a transfemoral arterial route, and is useful when the endoleak nidus communicates with the perigraft space [
23]. The transgraft approach uses direct puncture through the stent graft into the aneurysm sac; although technically feasible, it carries a risk of creating a new type III endoleak and is therefore generally reserved for cases in which no other access is available [
23]. In addition, a hybrid technique combining microsurgical–endovascular access via direct exposure and puncture of a lumbar segmental artery has been reported in a case not amenable to conventional endovascular access [
24], and laparoscopic clipping of the IMA or LAs remains a surgical alternative reserved for refractory endoleaks after multiple failed endovascular attempts [
25].
Embolic Materials
Selection of the embolic agent depends on the access route, the morphology of the endoleak, and operator experience.
Coils
Detachable and pushable microcoils remain the most widely used embolic agents, particularly for feeder vessel occlusion. They allow precise and controlled deployment but may be insufficient for nidus filling when used alone. Several studies have shown higher reintervention rates with coil-only embolization compared with liquid embolic materials [
11,
26,
27].
Liquid embolic agents have gained increasing prominence in T2EL embolization because of their ability to penetrate and fill the endoleak nidus and feeding vessels. The two most commonly used liquid agents are N-butyl cyanoacrylate (NBCA) and ethylene vinyl alcohol copolymer (Onyx).
NBCA (Histoacryl, B. Braun, Melsungen, Germany) is an adhesive liquid embolic that polymerizes rapidly upon contact with ionic environments, allowing rapid and durable sac occlusion at relatively low cost. The dilution ratio with ethiodized oil (Lipiodol, Guerbet, Villepinte, France) is typically tailored to the flow dynamics of the target endoleak and the number of feeding vessels. However, when multiple feeding vessels coexist within the endoleak nidus, the rapid polymerization of NBCA may result in early solidification of the embolic material before all feeders are occluded, leaving residual patent inflow channels that perpetuate the endoleak. Other major technical concerns include the risk of catheter retention and non-target embolization, both of which require careful technique and operator experience to mitigate [
28].
Onyx (Medtronic, Minneapolis, MN, USA) is a non-adhesive liquid embolic agent dissolved in dimethyl sulfoxide that precipitates upon contact with blood. Its non-adhesive nature allows controlled, prolonged injection and excellent penetration of the endoleak nidus and outflow vessels [
29]. However, the procedure is typically time-consuming, often requiring extended fluoroscopy time. In addition, because Onyx has a relatively high specific gravity and must be injected slowly (≤0.2 mL/min) to allow gradual polymerization, retrograde filling of the inflow arteries against arterial pressure can be difficult, and the agent tends to layer dependently within the sac rather than refluxing into upstream feeders.
In clinical practice, a combination of coils for feeder vessel occlusion and a liquid embolic for nidus filling is often advocated, particularly with direct sac puncture techniques. This combined approach addresses both inflow and outflow components of the endoleak and may reduce recurrence [
30].
Outcomes
A summary of representative outcome studies is provided in
Table 2 [
15,
21,
31-
35].
Routine post-embolization follow-up imaging is typically performed with contrast-enhanced CT (CE-CT). According to current guidelines, surveillance imaging is recommended within 1–6 months of the procedure and annually thereafter, with modifications based on residual endoleak status, sac size changes, and renal function [
10]. In patients with impaired renal function or contrast allergy in whom CE-CT is not feasible, non-contrast CT may be used to monitor changes in aneurysm sac diameter, or contrast-enhanced ultrasound (CE-US) with sulfur hexafluoride microbubbles (SonoVue, Bracco, Milan, Italy) may serve as a non-nephrotoxic alternative. CE-US offers several advantages, including the absence of nephrotoxicity (the microbubble contrast agent is eliminated via the lungs rather than the kidneys), the lack of ionizing radiation, and the ability to demonstrate real-time flow dynamics; pooled meta-analyses have reported sensitivities of approximately 91% for endoleak detection, comparable to CT angiography [
36].
Outcome reporting in T2EL embolization is heterogeneous, which complicates direct comparison across studies. The most commonly used endpoints are technical success defined as complete cessation of flow within the endoleak nidus and feeding vessels on completion angiography; radiological success defined as the absence of a visible endoleak on follow-up CE-CT; and clinical success defined as stabilization or shrinkage of the aneurysm sac on follow-up imaging, irrespective of residual endoleak.
Technical Success
Pooled technical success rates of T2EL embolization range from 84% to 100%, depending on the technique used [
32]. Direct sac puncture approaches generally yield higher technical success than TAAs. Hamidizadeh et al. [
32] reported a significantly higher technical success rate with TLA compared with TAA in a long-term study of 129 patients. For transabdominal direct sac puncture, Zener et al. [
15] reported a 100% technical success rate in 31 patients, and for TLA, reported technical success rates range from 90% to 100% across published series [
16-
18]. Transcaval approaches in recent series have achieved technical success rates of 96%–98% [
21,
34].
Clinical success rates vary widely (30%–90%), reflecting differences in definition, follow-up duration, embolic agent, and patient selection. Across direct sac puncture techniques, reported clinical success rates are approximately 81% for transabdominal embolization at 12 months [
15], 70%–85% for translumbar embolization [
16-
18], and up to 90% at 36 months for TCE [
34]. Long-term cohort data, however, have demonstrated a progressive decline in durability, with clinical success falling from approximately 82% at 12 months to 59% at 60 months [
35]. Larger registry analyses, including data from the Vascular Quality Initiative and the Japanese Committee for Stentgraft Management registry, have similarly confirmed that persistent T2EL is associated with sac enlargement and increased reintervention rates [
6,
37]. Notably, although persistent sac expansion is associated with higher rates of reintervention and open conversion, it does not appear to be independently associated with worse overall survival [
33,
35].
Direct comparisons of access routes have shown that the early advantage of TLA over TAA in technical success [
16] has narrowed in subsequent series using modified transarterial techniques, with comparable clinical success rates of 72%–78% reported between the two approaches [
18,
32]. With regard to embolic agents, Onyx has been associated with significantly lower reintervention rates than coils alone in long-term follow-up [
31]. Among direct sac puncture techniques, TCE has produced particularly favorable outcomes, with a pooled clinical success of 80% at 12 months [
21] and 90% at 36 months in a recent single-center series [
34].
Several patient-, procedural-, and imaging-related factors have been identified as influencing clinical success after T2EL embolization. From a procedural standpoint, Hamidizadeh et al. [
32] identified successful sac access during transarterial embolization and the use of NBCA glue as independent predictors of clinical success, with NBCA showing significantly higher success rates than other embolic agents (p = 0.017–0.037). Embolization of both the nidus and the feeding vessels—as opposed to feeder-only or nidus-only embolization—has also been associated with better long-term outcomes [
4,
11].
Imaging-based predictors are increasingly recognized. Pre-interventional CT findings such as unsharp or blurred T2EL delineation have been identified as predictors of persistent endoleak and continued sac expansion after embolization [
33]. Earlier work has also shown that CT features of T2EL flow dynamics can predict subsequent sac enlargement [
38]. These features include sharper delineation of the endoleak nidus on early arterial-phase CT angiography, persistent opacification across the venous and delayed phases, and a greater number and larger caliber of communicating branch vessels, all of which have been correlated with subsequent sac enlargement. Anatomic factors—a patent and large-caliber IMA, multiple patent LAs, and lower mural thrombus burden—are also associated with persistence and reduced response to embolization [
39,
40]. Such imaging- and anatomy-based predictors may help guide patient selection and inform decisions regarding alternative strategies, including open conversion in refractory cases.
Major complications are uncommon (<5%). Reported complications include non-target embolization (e.g., colonic ischemia, spinal cord injury), retroperitoneal hematoma, graft injury, infection, and—rarely—aneurysm rupture during or after the procedure [
27,
31].
Prophylactic Embolization
Given the limited durability of secondary embolization for established T2EL, prophylactic embolization of aortic side branches has emerged as a strategy to prevent T2EL after EVAR. Three main strategies have been described: selective IMA embolization-aneurysmal sac side branch (IMA-ASSB), in which a patent IMA is pre-emptively occluded with coils or a vascular plug before or during EVAR; non-selective aneurysmal sac side branch embolization (NS-ASSB), which combines IMA embolization with closure of patent LAs; and aneurysm sac coil embolization (ASCE), in which coils or a liquid embolic are placed directly within the aneurysm sac at the time of EVAR.
Rationale and Patient Selection
Anatomic predictors for T2EL include a patent IMA ≥3 mm in diameter, two or more patent LAs ≥2 mm in diameter, and an aortoiliac aneurysm configuration [
39,
40]. Patients with these features are considered high-risk for T2EL and may derive the greatest benefit from prophylactic embolization.
A landmark single-center randomized controlled trial evaluated pre-emptive IMA embolization in 106 high-risk patients with patent IMA and at least one additional anatomic risk factor (LAs ≥2 mm or aortoiliac configuration). At 5-year follow-up, the embolization group had significantly lower T2EL rates compared with controls (28.3% vs. 54.7%, p = 0.006), a higher freedom from sac enlargement, and a greater cumulative incidence of sac shrinkage [
41]. The multicenter CLARIFY-IMA study protocol has been initiated to further confirm these findings on a broader scale [
42].
Several recent systematic reviews and meta-analyses have consistently supported the efficacy of prophylactic side-branch embolization in reducing T2EL incidence, sac enlargement, and reintervention rates after EVAR compared with standard EVAR alone. These analyses, encompassing both retrospective cohort and updated randomized/registry data, have shown that all three strategies—IMA-ASSB, NS-ASSB, and ASCE—are superior to no embolization, with broadly comparable efficacy among them, although IMA-ASSB has shown a tendency toward better suppression of sac expansion and reintervention in network comparisons [
43-
47]. A summary of these key studies is provided in
Table 3 [
41,
43-
46].
Despite encouraging evidence, prophylactic embolization is not yet a standard of care. The ESVS 2024 guidelines acknowledge the accumulating data but note that broader implementation is not yet recommended without further high-quality evidence, including data on cost-effectiveness and the potential effect on rupture rates [
10]. Practical considerations include added procedural time, contrast load, radiation exposure, and procedural cost. However, selective application in high-risk patients—defined by anatomic criteria—appears to provide the most favorable risk-benefit ratio.
Conclusion
Type 2 endoleak embolization remains a clinically challenging but evolving field within interventional radiology. No single approach can be regarded as universally first-line; rather, the optimal access route—whether transarterial, transabdominal, translumbar, or transcaval—should be tailored to each patient based on the source vessel of the endoleak, sac location and anatomy, surrounding structures, prior intervention history, and patient-related factors such as positional tolerance. For IMA-dominant endoleaks with favorable SMA-IMA collateral, transarterial embolization remains an effective option, while direct sac puncture approaches are often more effective for LA-dominant or multi-source endoleaks. The transcaval approach has emerged as a particularly valuable option for sacs abutting the IVC and for cases in which prone positioning is contraindicated.
Liquid embolic agents, particularly Onyx and NBCA, have shown improved durability over coils alone, although optimal material selection remains individualized and dependent on the access route and endoleak morphology. Prophylactic embolization in carefully selected high-risk patients—supported by a recent randomized trial and multiple meta-analyses—appears to reduce T2EL incidence, sac enlargement, and reintervention rates. Nevertheless, its routine use is not yet endorsed by current guidelines.
In conclusion, we have summarized the current evidence on endovascular management of T2EL after EVAR. Multidisciplinary collaboration, careful patient selection, and tailored technique selection remain the cornerstones of successful management. Further prospective randomized trials with longer follow-up are needed to standardize practice and define the optimal role of each technique and embolic material.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Acknowledgments
None.
Data availability statement
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
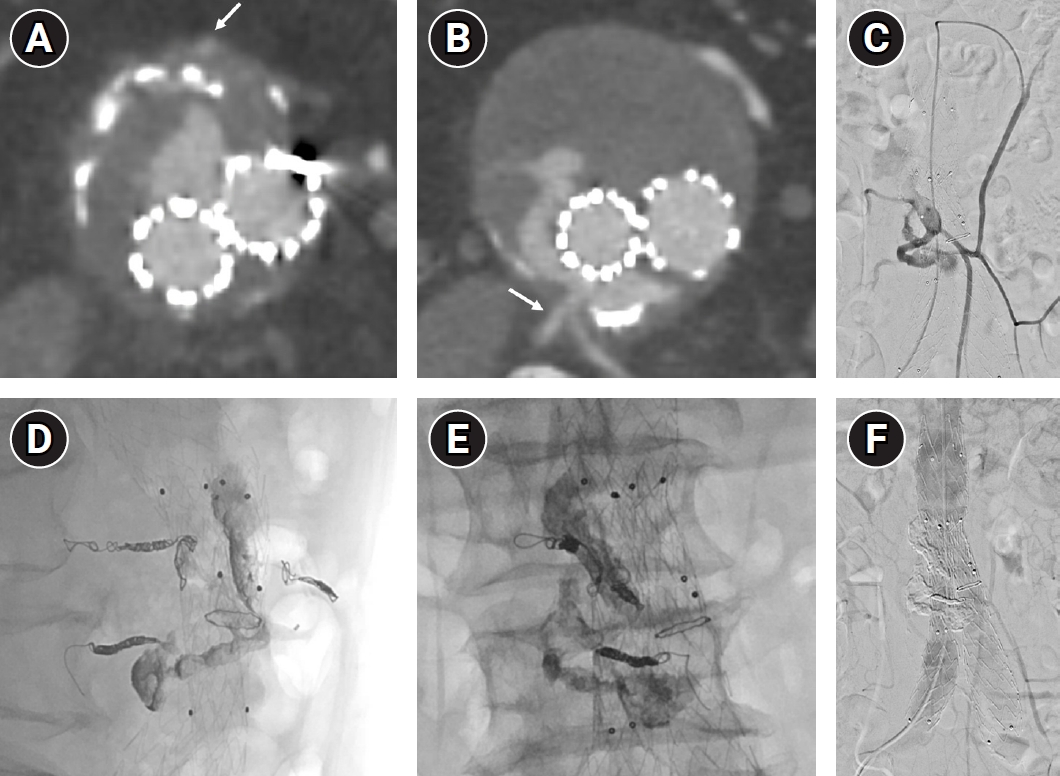
Fig. 1.Transarterial embolization of a type 2 endoleak via the SMA–arc of Riolan–inferior mesenteric artery (IMA) pathway in a 76-year-old man. (A) Axial CT image showing a type 2 endoleak fed by the inferior mesenteric artery (arrow). (B) Axial CT image at a more inferior level demonstrating additional feeding from bilateral lumbar arteries (arrow) connecting to the same endoleak nidus. (C) Selective superior mesenteric arteriography showing opacification of the IMA, endoleak nidus, and feeding lumbar arteries via the arc of Riolan. (D, E) Lateral (D) and anteroposterior (E) fluoroscopic images obtained after embolization of the IMA and lumbar arteries with coils and of the residual endoleak nidus with Onyx. (F) Post-embolization aortography demonstrating complete resolution of the type 2 endoleak.
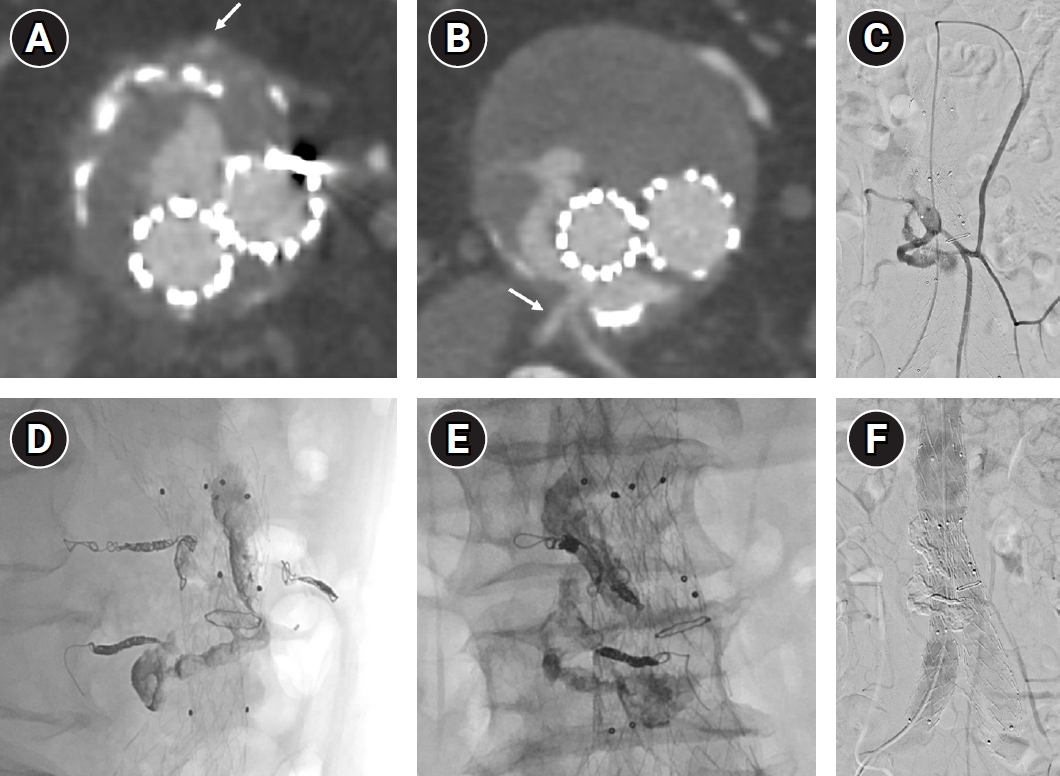
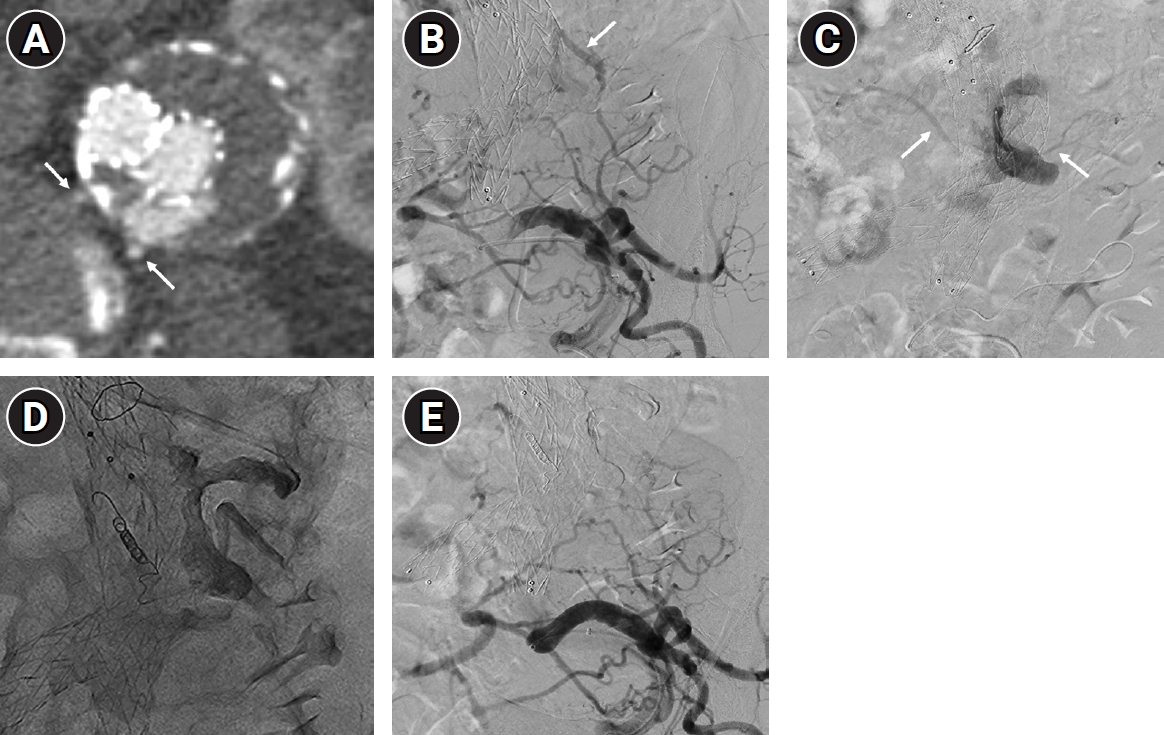
Fig. 2.Transarterial embolization of a type 2 endoleak via the internal iliac artery–iliolumbar collateral pathway in an 84-year-old woman. (A) Axial CT image showing a type 2 endoleak fed by bilateral lumbar arteries (arrows). (B) Left internal iliac arteriography demonstrating opacification of the endoleak nidus (arrow) through an iliolumbar collateral. (C) Angiography obtained after advancing a microcatheter through the iliolumbar collateral into the endoleak nidus, showing opacification of bilateral lumbar arteries (arrows). (D) Post-embolization image showing coil embolization of the right lumbar artery and Onyx embolization of the endoleak nidus and the left lumbar artery. (E) Final angiography demonstrating complete resolution of the type 2 endoleak.
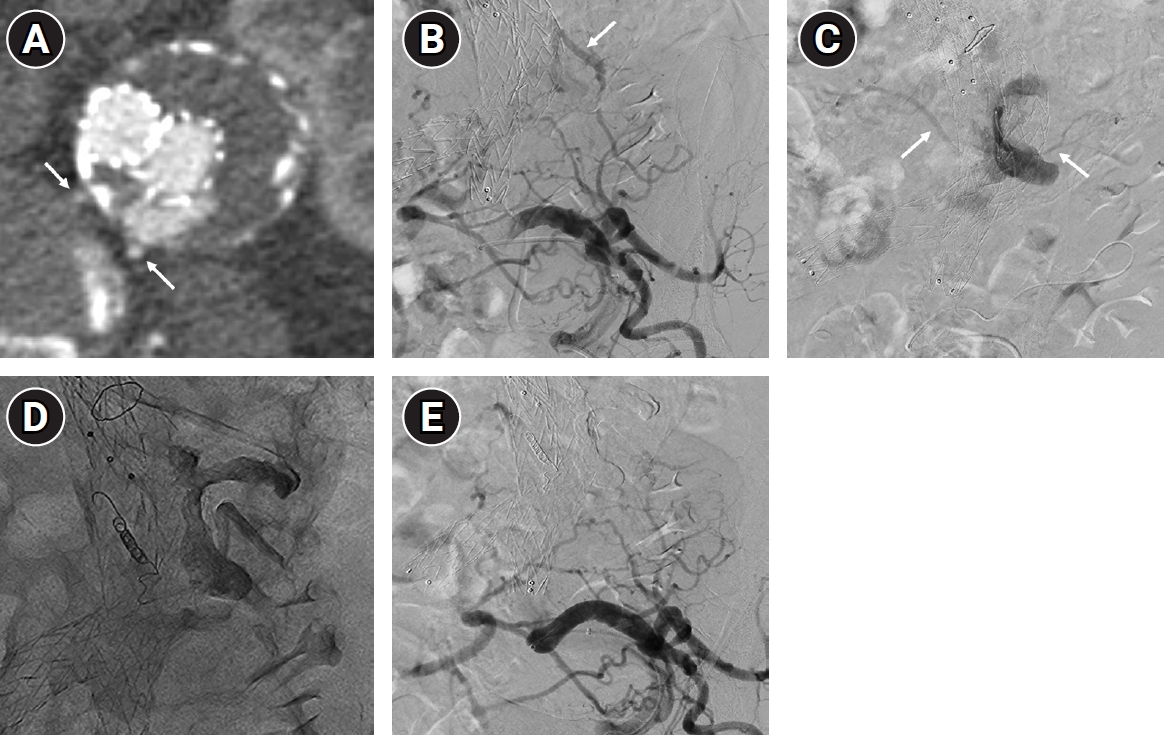
Fig. 3.Working assembly used for direct sac puncture embolization. A 4-Fr coaxial introducer sheath is connected to a Y-connector, allowing coaxial introduction of a microcatheter while maintaining hemostasis.
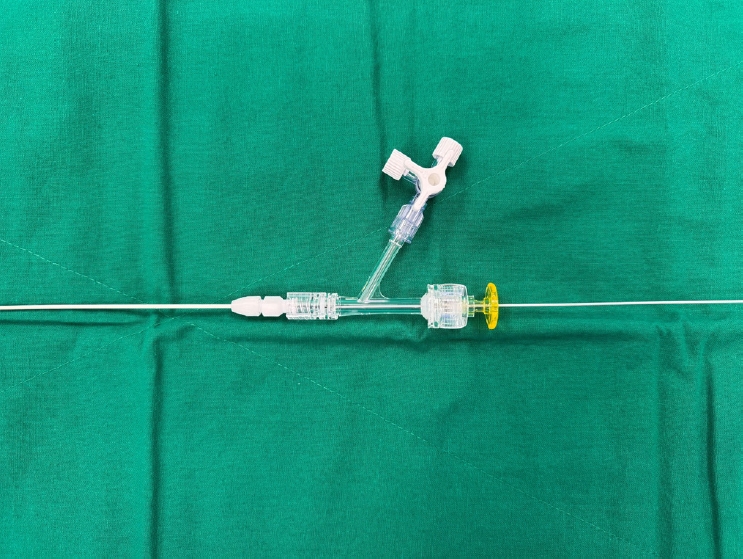
Fig. 4.Transabdominal direct sac puncture embolization of a type 2 endoleak in a 79-year-old woman. (A) Axial CT image showing a type 2 endoleak fed by a posteriorly arising lumbar artery (arrow) behind the aneurysm sac. (B) Selective angiography obtained after transabdominal direct sac puncture, demonstrating opacification of the endoleak nidus and bilateral lumbar arteries. (C) Post-embolization image showing coil embolization of the right lumbar artery and Onyx embolization of the residual endoleak nidus. (D) Follow-up CT image demonstrating complete resolution of the type 2 endoleak.
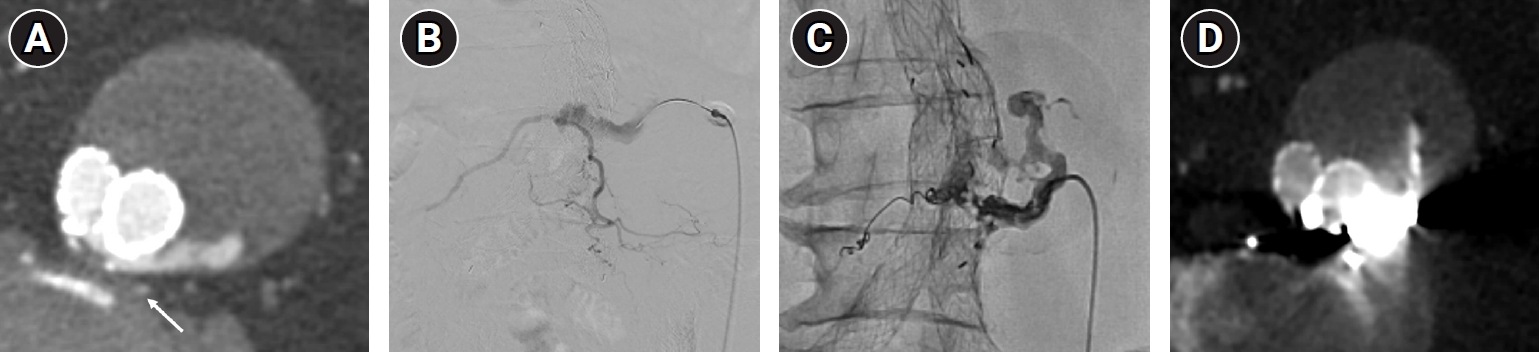
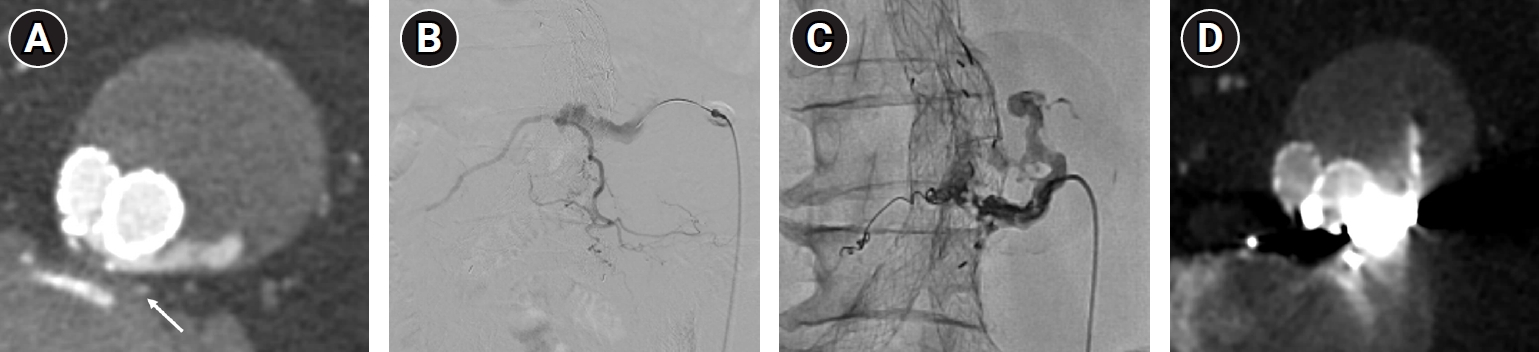
Fig. 5.Transcaval embolization of a type 2 endoleak in a 64-year-old man, in whom both transabdominal and translumbar approaches were precluded because the endoleak nidus was located between the stent-graft and the vertebral body. (A) Axial CT image showing a type 2 endoleak fed by a posteriorly arising lumbar artery (arrow), with the nidus positioned between the stent-graft and the vertebral body. (B) Fluoroscopic image showing transcaval puncture of the endoleak nidus using a Rösch-Uchida needle introduced via the right internal jugular vein. (C) Angiography obtained after intrasac access demonstrating opacification of the endoleak nidus and the feeding lumbar artery. (D) Post-embolization image showing complete obliteration of the endoleak nidus using N-butyl cyanoacrylate (NBCA) glue mixed with ethiodized oil at a 1:4 ratio.

Table 1.Comparison of approach techniques for type 2 endoleak embolization
Table 1.
|
Approach |
Advantages |
Limitations |
|
Transarterial |
Familiar technique |
Tortuous collateral pathway |
|
Supine position |
Lower technical success in lumbar-driven endoleaks |
|
Minimally invasive |
|
Transabdominal |
Direct sac access |
Risk of bowel/visceral injury |
|
Supine position |
Requires safe anterior window |
|
Ultrasound guided procedure |
|
Useful when sac is anteriorly located |
|
Translumbar |
Direct sac access |
Prone position |
|
Lower risk of bowel injury |
Risk of retroperitoneal hematoma |
|
Limited by kidney interposition |
|
Transcaval |
Supine position |
Risk of endograft injury |
|
Concurrent arterial access |
Aneurysm sac must abut to IVC |
Table 2.Summary of representative outcome studies of type 2 endoleak embolization
Table 2.
|
Study |
No. of patients |
Approach |
Embolic agent |
Technical success |
Clinical success |
|
Zener et al. (2018) [15] |
31 |
Transabdominal |
Coils, NBCA, Onyx |
100% |
81% |
|
Scallan et al. (2021) [31] |
58 |
TAA/TLA |
Onyx vs. coils |
Not reported |
Lower reintervention with Onyx |
|
Hamidizadeh et al. (2021) [32] |
129 |
TAA vs. TLA |
NBCA, coils, Onyx |
Higher with TLA |
NBCA superior; access success a predictor |
|
Nana et al. (2022, SR) [21] |
117 |
Transcaval |
Various |
Pooled 96% |
80% at 12 months |
|
Vandenbulcke et al. (2023) [33] |
60 |
TAA/TLA |
Various |
95% |
Radiological 26.7%; sac stable in 48.3% |
|
Nana et al. (2024) [34] |
43 |
Transcaval |
Coils, Onyx |
97.7% |
90% at 36 months |
|
Chun et al. (2026) [35] |
72 |
Mixed |
Various |
77% |
82%/70%/59% at 12/24/60 months |
Table 3.Summary of representative studies on prophylactic embolization to prevent type 2 endoleak
Table 3.
|
Author (Year) |
Design |
Strategy |
T2EL rate (Emb vs. Ctrl) |
Reintervention (Emb vs. Ctrl) |
|
Yu et al. (2020) [43] |
Meta-analysis |
Side-branch embolization |
18.5% vs. 38.6% (OR 0.34) |
1.5% vs. 12.4% (OR 0.12) |
|
Yu et al. (2023) [44] |
Meta-analysis |
Side-branch embolization |
Reduced T2EL (OR 0.40) |
Reduced |
|
Takeuchi et al. (2024) [41] |
Single-center RCT |
IMA embolization |
28.3% vs. 54.7% (p = 0.006) |
Reduced |
|
Niklas et al. (2022) [45] |
Meta-analysis |
IMA embolization |
Reduced T2EL incidence |
Reduced |
|
Wu et al. (2022) [46] |
Meta-analysis |
IMA-ASSB vs. NS-ASSB vs. ASCE |
All strategies superior to no embolization |
IMA-ASSB tended to lower reintervention |
References
- 1. White GH, Yu W, May J, Chaufour X, Stephen MS. Endoleak as a complication of endoluminal grafting of abdominal aortic aneurysms: classification, incidence, diagnosis, and management. J Endovasc Surg. 1997;4:152-168. https://doi.org/10.1177/152660289700400207
- 2. Baum RA, Stavropoulos SW, Fairman RM, Carpenter JP. Endoleaks after endovascular repair of abdominal aortic aneurysms. J Vasc Interv Radiol. 2003;14:1111-1117. https://doi.org/10.1097/01.rvi.0000085773.71254.86
- 3. Rhee SJ, Ohki T, Veith FJ, Kurvers H. Current status of management of type II endoleaks after endovascular repair of abdominal aortic aneurysms. Ann Vasc Surg. 2003;17:335-344. https://doi.org/10.1007/s10016-003-0002-5
- 4. Chuter TA, Faruqi RM, Sawhney R, Reilly LM, Kerlan RB, Canto CJ, et al. Endoleak after endovascular repair of abdominal aortic aneurysm. J Vasc Surg. 2001;34:98-105. https://doi.org/10.1067/mva.2001.111487
- 5. Pineda DM, Calligaro KD, Tyagi S, Troutman DA, Dougherty MJ. Late type II endoleaks after endovascular aneurysm repair require intervention more frequently than early type II endoleaks. J Vasc Surg. 2018;67:449-452. https://doi.org/10.1016/j.jvs.2017.05.124
- 6. Seike Y, Matsuda H, Shimizu H, Ishimaru S, Hoshina K, Michihata N, et al. Nationwide analysis of persistent type II endoleak and late outcomes of endovascular abdominal aortic aneurysm repair in Japan: a propensity-matched analysis. Circulation. 2022;145:1056-1066. https://doi.org/10.1161/CIRCULATIONAHA.121.056581
- 7. Iwakoshi S, Ogawa Y, Dake MD, Ono Y, Higashihara H, Ikoma A, et al. Outcomes of embolization procedures for type II endoleaks following endovascular abdominal aortic repair. J Vasc Surg. 2023;77:114-121. https://doi.org/10.1016/j.jvs.2022.07.168
- 8. Ultee KH, Buttner S, Huurman R, Bastos Goncalves F, Hoeks SE, Bramer WM, et al. Editor's choice: systematic review and meta-analysis of the outcome of treatment for type II endoleak following endovascular aneurysm repair. Eur J Vasc Endovasc Surg. 2018;56:794-807. https://doi.org/10.1016/j.ejvs.2018.06.009
- 9. Chaikof EL, Dalman RL, Eskandari MK, Jackson BM, Lee WA, Mansour MA, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018;67:2-77. https://doi.org/10.1016/j.jvs.2017.10.044
- 10. Wanhainen A, Van Herzeele I, Bastos Goncalves F, Bellmunt Montoya S, Berard X, Boyle JR, et al. Editor's choice: European Society for Vascular Surgery (ESVS) 2024 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2024;67:192-331. https://doi.org/10.1016/j.ejvs.2023.11.002
- 11. Sarac TP, Gibbons C, Vargas L, Liu J, Srivastava S, Bena J, et al. Long-term follow-up of type II endoleak embolization reveals the need for close surveillance. J Vasc Surg. 2012;55:33-40. https://doi.org/10.1016/j.jvs.2011.07.092
- 12. Onishi Y, Shimizu H, Kawatou M, Minatoya K, Nakamoto Y. Transarterial embolization of type 2 endoleak post thoracic endovascular aortic repair (TEVAR) using a triaxial system with a 1.3-F microcatheter: a case report. Cureus. 2024;16:e51694. https://doi.org/10.7759/cureus.51694
- 13. Yang RY, Tan KT, Beecroft JR, Rajan DK, Jaskolka JD. Direct sac puncture versus transarterial embolization of type II endoleaks: an evaluation and comparison of outcomes. Vascular. 2017;25:227-233. https://doi.org/10.1177/1708538116663992
- 14. Burke CT, Yu H. How I do it: computed tomography-guided modified translumbar embolization of type 2 endoleak. Semin Intervent Radiol. 2021;38:576-580. https://doi.org/10.1055/s-0041-1736656
- 15. Zener R, Oreopoulos G, Beecroft R, Rajan DK, Jaskolka J, Tan KT. Transabdominal direct sac puncture embolization of type II endoleaks after endovascular abdominal aortic aneurysm repair. J Vasc Interv Radiol. 2018;29:1167-1173. https://doi.org/10.1016/j.jvir.2018.04.002
- 16. Baum RA, Carpenter JP, Golden MA, Velazquez OC, Clark TW, Stavropoulos SW, et al. Treatment of type 2 endoleaks after endovascular repair of abdominal aortic aneurysms: comparison of transarterial and translumbar techniques. J Vasc Surg. 2002;35:23-29. https://doi.org/10.1067/mva.2002.121068
- 17. Stavropoulos SW, Carpenter JP, Fairman RM, Golden MA, Baum RA. Inferior vena cava traversal for translumbar endoleak embolization after endovascular abdominal aortic aneurysm repair. J Vasc Interv Radiol. 2003;14:1191-1194. https://doi.org/10.1097/01.rvi.0000085771.71254.14
- 18. Stavropoulos SW, Park J, Fairman R, Carpenter J. Type 2 endoleak embolization comparison: translumbar embolization versus modified transarterial embolization. J Vasc Interv Radiol. 2009;20:1299-1302. https://doi.org/10.1016/j.jvir.2009.07.003
- 19. Mansueto G, Cenzi D, Scuro A, Gottin L, Griso A, Gumbs AA, et al. Treatment of type II endoleak with a transcatheter transcaval approach: results at 1-year follow-up. J Vasc Surg. 2007;45:1120-1127. https://doi.org/10.1016/j.jvs.2007.01.063
- 20. Giles KA, Fillinger MF, De Martino RR, Hoel AW, Powell RJ, Walsh DB. Results of transcaval embolization for sac expansion from type II endoleaks after endovascular aneurysm repair. J Vasc Surg. 2015;61:1129-1136. https://doi.org/10.1016/j.jvs.2014.12.002
- 21. Nana P, Spanos K, Heidemann F, Panuccio G, Kouvelos G, Rohlffs F, et al. Systematic review on transcaval embolization for type II endoleak after endovascular aortic aneurysm repair. J Vasc Surg. 2022;76:282-291. https://doi.org/10.1016/j.jvs.2022.02.032
- 22. Van Sickler AP, Smith AH, Ellis RC, Steenberge SP, Quatromoni JG, Rowse JW, et al. A novel technique and outcomes for transcaval endoleak embolization. Ann Vasc Surg. 2023;93:300-307. https://doi.org/10.1016/j.avsg.2023.01.013
- 23. Chen JX, Stavropoulos SW. Type 2 endoleak management. Semin Intervent Radiol. 2020;37:365-370. https://doi.org/10.1055/s-0040-1715873
- 24. Nguyen VN, Rennert RC, Sternbach S, Cavaleri J, Abedi A, Atai NA, et al. A novel combined microsurgical and endovascular approach for type II endoleak embolization through direct puncture of a lumbar segmental artery: a technical case instruction. Neurosurg Pract. 2024;5:e00115. https://doi.org/10.1227/neuprac.0000000000000115
- 25. Spanos K, Tsilimparis N, Larena-Avellaneda A, Giannoukas AD, Debus SE, Kölbel T. Systematic review of laparoscopic ligation of inferior mesenteric artery for the treatment of type II endoleak after endovascular aortic aneurysm repair. J Vasc Surg. 2017;66:1878-1884. https://doi.org/10.1016/j.jvs.2017.07.066
- 26. Stavropoulos SW, Kim H, Clark TW, Fairman RM, Velazquez O, Carpenter JP. Embolization of type 2 endoleaks after endovascular repair of abdominal aortic aneurysms with use of cyanoacrylate with or without coils. J Vasc Interv Radiol. 2005;16:857-861. https://doi.org/10.1097/01.RVI.0000156495.66062.62
- 27. Abularrage CJ, Patel VI, Conrad MF, Schneider EB, Cambria RP, Kwolek CJ. Improved results using Onyx glue for the treatment of persistent type 2 endoleak after endovascular aneurysm repair. J Vasc Surg. 2012;56:630-636. https://doi.org/10.1016/j.jvs.2012.02.038
- 28. Kajiwara K, Yamagami T, Urashima M, Tomiyoshi H, Kakizawa H, Yoshimatsu R, et al. Embolization for type 2 endoleak with sac expansion after endovascular repair of abdominal aortic aneurysm: safety and effectiveness. Springerplus. 2016;5:262. https://doi.org/10.1186/s40064-016-1934-x
- 29. Massis K, Carson WG 3rd, Rozas A, Patel V, Zwiebel B. Treatment of type II endoleaks with ethylene-vinyl-alcohol copolymer (Onyx). Vasc Endovascular Surg. 2012;46:251-257. https://doi.org/10.1177/1538574412442401
- 30. Khaja MS, Park AW, Swee W, Evans AJ, Fritz Angle J, Turba UC, et al. Treatment of type II endoleak using Onyx with long-term imaging follow-up. Cardiovasc Intervent Radiol. 2014;37:613-622. https://doi.org/10.1007/s00270-013-0706-z
- 31. Scallan O, Kribs S, Power AH, DeRose G, Duncan A, Dubois L. Onyx versus coil embolization for the treatment of type II endoleaks. J Vasc Surg. 2021;73:1966-1972. https://doi.org/10.1016/j.jvs.2020.10.069
- 32. Hamidizadeh R, Nzekwu E, Halliwell O. Factors influencing clinical success following endovascular treatment of type II endoleaks. Can Assoc Radiol J. 2021;72:890-897. https://doi.org/10.1177/0846537120981100
- 33. Vandenbulcke R, Houthoofd S, Laenen A, Buyck PJ, Mufty H, Fourneau I, et al. Embolization therapy for type 2 endoleaks after endovascular aortic aneurysm repair: imaging-based predictive factors and clinical outcomes on long-term follow-up. Diagn Interv Radiol. 2023;29:331-341. https://doi.org/10.4274/dir.2022.22352
- 34. Nana P, Panuccio G, Rohlffs F, Torrealba JI, Spanos K, Kolbel T. Early and mid-term outcomes of transcaval embolization for type 2 endoleak after endovascular aortic repair. J Clin Med. 2024;13:3578. https://doi.org/10.3390/jcm13123578
- 35. Chun JY, Patel S, Ameli-Renani S, Pavlidis V, Morgan R. Embolisation of type 2 endoleaks associated with sac expansion: outcomes from a single-centre cohort. Cardiovasc Intervent Radiol. 2026;49:496-507. https://doi.org/10.1007/s00270-025-04272-8
- 36. Bredahl KK, Taudorf M, Lonn L, Vogt KC, Sillesen H, Eiberg JP. Contrast enhanced ultrasound can replace computed tomography angiography for surveillance after endovascular aortic aneurysm repair. Eur J Vasc Endovasc Surg. 2016;52:729-734. https://doi.org/10.1016/j.ejvs.2016.07.007
- 37. DeMartino RR, Breite MD, Neal D, Mendes BC, Colglazier JJ, Stone DH, et al. Incidence, reintervention, and survival associated with type II endoleak at hospital discharge after elective endovascular aneurysm repair in the Vascular Quality Initiative. J Vasc Surg. 2023;78:679-686.e1. https://doi.org/10.1016/j.jvs.2023.05.041
- 38. Muller-Wille R, Schotz S, Zeman F, Uller W, Guntner O, Pfister K, et al. CT features of early type II endoleaks after endovascular repair of abdominal aortic aneurysms help predict aneurysm sac enlargement. Radiology. 2015;274:906-916. https://doi.org/10.1148/radiol.14140284
- 39. Ward TJ, Cohen S, Patel RS, Kim E, Fischman AM, Nowakowski FS, et al. Anatomic risk factors for type-2 endoleak following EVAR: a retrospective review of preoperative CT angiography in 326 patients. Cardiovasc Intervent Radiol. 2014;37:324-328. https://doi.org/10.1007/s00270-013-0646-7
- 40. Jones JE, Atkins MD, Brewster DC, Chung TK, Kwolek CJ, LaMuraglia GM, et al. Persistent type 2 endoleak after endovascular repair of abdominal aortic aneurysm is associated with adverse late outcomes. J Vasc Surg. 2007;46:1-8. https://doi.org/10.1016/j.jvs.2007.02.073
- 41. Takeuchi Y, Morikage N, Samura M, Sakamoto R, Ike S, Mizoguchi T, et al. Five-year follow-up of randomized clinical trial for pre-emptive inferior mesenteric artery embolization during endovascular aneurysm repair. J Vasc Surg. 2024;80:693-701. https://doi.org/10.1016/j.jvs.2024.04.058
- 42. Ichihashi S, Takahara M, Fujimura N, Nagatomi S, Iwakoshi S, Bolstad F, et al. Multicentre randomised controlled trial to evaluate the efficacy of pre-emptive inferior mesenteric artery embolisation during endovascular aortic aneurysm repair on aneurysm sac change: protocol of Clarify IMA study. BMJ Open. 2020;10:e031758. https://doi.org/10.1136/bmjopen-2019-031758
- 43. Yu HY, Lindstrom D, Wanhainen A, Tegler G, Hassan B, Mani K. Systematic review and meta-analysis of prophylactic aortic side branch embolization to prevent type II endoleaks. J Vasc Surg. 2020;72:1783-1792. https://doi.org/10.1016/j.jvs.2020.05.020
- 44. Yu HY, Lindstrom D, Wanhainen A, Tegler G, Asciutto G, Mani K. An updated systematic review and meta-analysis of pre-emptive aortic side branch embolization to prevent type II endoleaks after endovascular aneurysm repair. J Vasc Surg. 2023;77:1815-1821. https://doi.org/10.1016/j.jvs.2022.11.042
- 45. Niklas N, Malec M, Gutowski P, Kazimierczak A, Rynio P. Effectiveness of inferior mesenteric artery embolization on type II endoleak-related complications after endovascular aortic repair (EVAR): systematic review and meta-analysis. J Clin Med. 2022;11:5491. https://doi.org/10.3390/jcm11185491
- 46. Wu Y, Yin J, Hongpeng Z, Wei G. Systematic review and network meta-analysis of pre-emptive embolization of the aneurysm sac side branches and aneurysm sac coil embolization to improve the outcomes of endovascular aneurysm repair. Front Cardiovasc Med. 2022;9:947809. https://doi.org/10.3389/fcvm.2022.947809
- 47. Chen Q, Zhang Y, Lei K, Fu L, Zhang D, Sun W, et al. Efficacy and safety of prophylactic intraoperative sac embolization in EVAR for abdominal aortic aneurysm: a meta-analysis. Front Surg. 2022;9:1027231. https://doi.org/10.3389/fsurg.2022.1027231