Abstract
-
Purpose
This study aims to investigate the clinical outcomes and safety of a standardized two-session catheter-directed ethanol sclerotherapy protocol for peritoneal inclusion cysts.
-
Materials and Methods
Between November 2020 and July 2025, six women (median age, 32.5 years) with symptomatic peritoneal inclusion cysts underwent ethanol sclerotherapy. After complete drainage using an 8.5-Fr or 10.2-Fr pigtail catheter, two sessions of sclerotherapy were performed on consecutive days. In each session, 99.5% ethanol (50% of the aspirated volume, up to 150 mL) was instilled and retained for 20 minutes. Follow-up ultrasound was performed at 1, 3, and 6 months. Technical success was defined as successful completion of both sessions with a 20-minute ethanol retention time, and clinical success was defined as symptom improvement with a >50% decrease in cyst diameter at 3 months.
-
Results
Technical success was achieved in all cases (6/6, 100%). The median maximum cyst diameter significantly decreased from 14.0 cm (range, 6.0 to 20.0 cm) to 5.25 cm (range, 2.0 to 8.0 cm) at the follow-up within 1 month (p = 0.03). Clinical success was achieved in all cases at 3 months (6/6, 100%). No residual cysts were visualized on follow-up ultrasound at 6 months in all patients (6/6, 100%). Anti-Müllerian hormone levels measured in four patients showed heterogeneous changes, precluding definitive conclusions regarding the impact on ovarian reserve. No major complications occurred.
-
Conclusion
Two-session catheter-directed ethanol sclerotherapy appears to be a safe and effective minimally invasive alternative to surgery for peritoneal inclusion cysts, providing a high rate of complete resolution.
-
Keywords: Peritoneal inclusion cysts; Ethanol; Sclerotherapy; Drainage; Catheterization
Introduction
Peritoneal inclusion cysts (PICs) are variably sized, mesothelial-lined cysts located within the abdominopelvic cavity. PICs are thought to arise secondary to intra-abdominal inflammation and subsequent cyst formation, with serous fluid originating from the ovarian stroma [
1]. Patients typically present with progressive abdominal or pelvic pain and/or a palpable abdominal mass. PICs generally contain clear to yellow serous fluid; however, they may also contain hemorrhagic or gelatinous, discolored fluid [
1]. Under normal physiological conditions, peritoneal fluid is produced by the ovaries and resorbed by the peritoneal surface [
2]. The absorptive capacity of the peritoneal surface can be impaired, and an inflammatory exudate may develop due to benign reactions to prior pelvic or abdominal surgery, pelvic inflammatory disease, endometriosis, or inflammatory bowel disease during the third or fourth decade of life, leading to impaired peritoneal resorption [
1,
3,
4]. Inflammatory reactions surrounding surgical interventions may lead to the encapsulation of peritoneal fluid, while increased fluid volumes can stimulate PIC formation.
Pharmacological treatment primarily provides symptomatic relief and lacks a permanent curative effect. This poses challenges for patients wishing to preserve their fertility, as long-term medication use may have adverse implications [
1]. While surgical resection remains the conventional approach, it is frequently hampered by dense postoperative adhesions and a high recurrence rate of up to 50%. Furthermore, repeated surgical trauma can exacerbate peritoneal dysfunction [
5]. Thus, there is a critical need for a standardized, minimally invasive strategy that ensures long-term success while minimizing surgical morbidity. Simple needle aspiration provides a safe and straightforward method for fluid analysis and symptom management; however, it is almost invariably followed by rapid fluid re-accumulation [
1]. Consequently, image-guided sclerotherapy has emerged as a minimally invasive alternative aimed at achieving permanent closure of the cystic space through the induction of mesothelial fibrosis. Nonetheless, the efficacy of sclerotherapy may be hindered by the multiloculated structure of PICs, which can obstruct the sclerosing agent from effectively reaching all sequestered compartments. Traditional sclerotherapy protocols for PICs have been inconsistent, ranging from single-needle aspirations with high recurrence rates to prolonged catheter-based regimens requiring excessive instillations (mean >3 sessions) and varying sclerosing agents [
6,
7]. To enhance treatment efficacy while minimizing procedural burden and chemical irritation, we hypothesized that a standardized two-session catheter-directed ethanol sclerotherapy protocol could reduce the number of instillations and total hospitalization duration compared to conventional multi-session approaches, while maintaining comparable treatment efficacy. Herein, we report the clinical outcomes and safety of this standardized protocol as a preliminary case series. The term “preliminary” refers to the small patient cohort and relatively short follow-up duration, and specifically reflects our initial clinical experience with this particular standardized two-session protocol and its associated outcome measures, rather than the broader concept of sclerotherapy for PICs, which has been previously reported in the literature.
Materials and Methods
Due to the retrospective nature of this study, the requirement for informed consent was waived by the institutional review board (S2026-0227-0001). This study was conducted in accordance with the Declaration of Helsinki. Between November 2020 and July 2025, six women who were referred by gynecologists underwent a standardized two-session catheter-directed ethanol sclerotherapy protocol for PICs. All patients presented with pelvic pain (n = 5) or a sensation of fullness (n = 1). The median age of the patients was 32.5 years (range, 23 to 48 years). Each patient had a diverse surgical history in the abdominopelvic region (
Table 1). The median interval between the previous surgery and sclerotherapy was 14.5 years (range, 1.75 to 28 years). PIC was diagnosed based on clinical history and characteristic findings on ultrasound, CT, or MRI. Imaging features included a multiloculated cystic pelvic mass with thin septations, absence of solid components or internal vascularity on Doppler imaging, and close apposition to the ovary, reflecting entrapped peritoneal fluid within adhesions. Other cystic pelvic lesions, including ovarian cystadenomas, endometriomas, hydrosalpinx, and lymphoceles, were excluded based on their characteristic imaging features (e.g., solid components, high internal echogenicity suggestive of hemorrhagic content, tubular configuration, or typical postoperative location) in conjunction with clinical history. Malignancy was excluded based on imaging findings and tumor markers, including cancer antigen 125, human epididymis protein 4, and the Risk of Ovarian Malignancy Algorithm.
For the transabdominal percutaneous approach (
Figs. 1,
2), the puncture site was first disinfected with povidone-iodine (Betadine, Mundipharma, Basel, Switzerland), and the target lesion was punctured with a 21-gauge, 15-cm Chiba needle (Cook Medical, Bloomington, IN, USA) using a freehand technique. Subsequently, a 0.018-in guidewire (Cook Medical) and a Neff Percutaneous Access Set (Cook Medical) were introduced, and a 0.035-in hydrophilic guidewire (Terumo, Tokyo, Japan) was advanced under fluoroscopic guidance.
In cases requiring a transvaginal approach (
Fig. 3), patients were positioned in the lithotomy position. The vaginal area was sterilized with a 0.5% chlorhexidine gluconate solution (Hexitane 0.5%, Firson, Cheonan, Korea). An ultrasound probe with an in-plane endocavitary needle guide (EVN4-9, Aspen Surgical, Caledonia, MI, USA) was inserted. The lesion was punctured using an 18-gauge, 20-cm Chiba biopsy needle (Cook Medical), and a 0.035-in hydrophilic guidewire (Terumo) was advanced into the cyst.
Regardless of the chosen access route, the guidewire was advanced as far as possible to allow adequate coiling within the cyst cavity. Following guidewire placement, an 8.5- or 10.2-Fr pigtail drainage catheter with multiple side holes (Dawson-Mueller Drainage Catheter, Cook Medical) was inserted over the wire.
Following complete aspiration of the cyst contents, the cavity was filled with 10–30 mL of a water-soluble nonionic contrast medium (iobitridol, Xenetix 300 [300 mg I/mL], Guerbet, Villepinte, France) to assess for any leakage into the pelvic cavity (
Figs. 1–
3). Once the contrast medium was aspirated, the cyst was irrigated with 10–30 mL of lidocaine to alleviate procedural discomfort and then completely aspirated. This was followed by irrigation with 10–30 mL of 99.5% anhydrous ethanol (Taiwan Biotech Co., Ltd., Taoyuan, Taiwan) to ensure the purity of the subsequent sclerotherapy; this pre-wash ethanol was also completely aspirated before therapeutic ethanol was instilled for retention. The cyst was then filled with 99.5% ethanol for retention; the administered volume was equivalent to 50% of the aspirated fluid, with an initial predefined maximum limit of 100 mL. In cyst sclerotherapy, ethanol volume is typically determined as a proportion of the aspirated volume to ensure adequate mucosal contact while minimizing the risk of systemic absorption. Patient pain tolerance was additionally used as a real-time safety parameter, as intraprocedural pain may indicate peritoneal irritation. In the final two patients with larger cysts, the maximum volume was increased to 150 mL based on acceptable pain tolerance and the absence of clinical signs of peritoneal irritation, in order to improve ethanol-cyst wall contact. This represents a within-study protocol modification. To optimize contact between the ethanol and the cyst wall, the catheter was clamped, and the patient was instructed to rotate through the supine, bilateral decubitus, and prone positions every 5 minutes. After 20 minutes, the ethanol was aspirated as thoroughly as possible, and the catheter was left in situ overnight for a second session on the following day. The two-session design was based on the rationale that a second ethanol instillation the following day would treat any residual viable mesothelium exposed after initial cyst collapse, thereby maximizing obliteration of the secreting surface while limiting the total procedural burden to a single hospitalization [
8,
9]. The 20-minute retention time was selected in accordance with previously established protocols for ethanol sclerotherapy of ovarian cysts, which have demonstrated sufficient contact time for mesothelial destruction without increasing the risk of systemic absorption [
10,
11]. On the following day, after reconfirming the absence of leakage, the second session was performed according to the same standardized protocol, using identical irrigation volumes and a 20-minute ethanol retention time. Upon completion, the catheter was removed, and the patient was monitored for complications prior to discharge on the same day. The procedure was terminated if contrast leakage or intolerable pain occurred. An aliquot of the drained fluid was submitted for cytological examination to exclude malignancy.
For pain management, intracystic lidocaine irrigation (10–30 mL) was used for intraprocedural analgesia, as described above. No routine systemic analgesics or conscious sedation were administered prior to or during the procedure. Additional systemic analgesics (e.g., nonsteroidal anti-inflammatory drugs) were provided on an as-needed basis for postprocedural discomfort during the inpatient stay. Prophylactic antibiotics were not routinely administered.
Definitions and Analysis
Participants were regularly monitored with ultrasound within 1 month (range, 15 to 30 days) and at 3 and 6 months following catheter-directed ethanol sclerotherapy to assess changes in cyst diameter, complications, and recurrence. To evaluate the impact of catheter-directed ethanol sclerotherapy on ovarian reserve, serum anti-Müllerian hormone (AMH) levels were measured within 1 week prior to the procedure and at 3 and 6 months after the procedure, when available.
Technical success was defined as the successful completion of both sessions, with ethanol retained inside the cyst for 20 minutes during each session. Clinical success was characterized by symptomatic improvement and a >50% decrease in cyst diameter at 3 months post-procedure. Symptomatic improvement was assessed using patient-reported outcomes at each follow-up visit, with patients reporting whether their presenting symptoms (pelvic pain or sensation of fullness) had resolved or persisted compared with baseline. Recurrence was defined as the enlargement of the treated PICs on ultrasound during follow-up. Major complications were defined as procedure-related adverse events that caused or prolonged hospitalization, required an invasive procedure for treatment, or resulted in a change in functional status. Minor complications were defined as transient procedure-related adverse events requiring nominal or no treatment, with or without overnight hospitalization for observation, and that resolved spontaneously [
12].
Continuous variables were expressed as the mean ± standard deviation or median with range, as appropriate, and categorical variables as frequencies and percentages. Changes in maximum cyst diameter between baseline and the first follow-up examination within 1 month after sclerotherapy were assessed using the Wilcoxon signed-rank test. A two-sided p < 0.05 was considered statistically significant. All statistical analyses were conducted using SPSS version 26.0 (IBM Corp., Armonk, NY, USA).
Results
A total of six lesions within the pelvic cavity were treated in six patients. The median pre-procedural maximum diameter of the PICs was 14.0 cm (range, 6.0 to 20.0 cm). Access routes were determined based on the cyst location: transvaginal access was employed in one patient (case 4) to avoid the risk of bowel injury, as the transabdominal route was not feasible owing to overlying bowel loops (
Fig. 3), while transabdominal access was utilized in the remaining five patients (
Figs. 1,
2). For drainage, 8.5-Fr pigtail catheters were used in five patients. However, case 6 required a 10.2-Fr catheter over a guidewire due to inadequate aspiration with the initial catheter (
Fig. 2). The median volume of aspirated fluid was 670 mL, which ranged widely (range, 85 to 1,060 mL). The aspirated fluid was predominantly straw-colored and low-viscosity, except for a darkish, thin fluid in case 1. Cytological analysis of all aspirated fluid specimens was negative for malignant cells.
The volume of ethanol instilled per session ranged from 42 to 150 mL. Technical success was achieved in all cases (100%). Patients were admitted for a scheduled three-day stay, with the first session performed on the day after admission (day 2) and the second session performed on the next morning (day 3), followed by immediate discharge.
Follow-up ultrasound imaging within 1 month demonstrated a marked reduction in cyst size in all patients (
Figs. 1–
3), with the maximum PIC diameter decreasing from a median of 14.0 cm (range, 6.0 to 20.0 cm) to 5.25 cm (range, 2.0 to 8.0 cm) (p = 0.03). At the 3-month follow-up, the cysts were no longer visible in five patients, and in one patient (case 1), the cyst diameter had decreased to 1.8 cm, meeting the criteria for clinical success (
Fig. 1). All patients reported resolution of their presenting symptoms at the 3-month follow-up, including pelvic pain in five patients and a sensation of pelvic fullness in one patient. By the 6-month follow-up, no visible cysts remained in any of the patients, confirming sustained resolution and no recurrence in all patients.
No major complications, such as chemical peritonitis, hemorrhage, or bowel injury, were observed; minor complications were limited to transient intraprocedural pain, which resolved with conservative analgesia. AMH levels were available for four patients; levels increased in two patients and decreased in the other two following the procedure.
Discussion
PICs are benign but often symptomatic lesions that predominantly affect premenopausal women with a history of pelvic surgery or inflammation [
1]. While surgical resection has traditionally been the primary treatment, high recurrence rates and the risk of adhesion formation have prompted the investigation of less invasive alternatives. This study suggests that ultrasound-guided ethanol sclerotherapy, performed in two sessions, may represent a promising treatment option for PICs in this preliminary series, showing a marked reduction in cyst size within the first month and cyst disappearance in all patients at 6 months. However, given that follow-up was primarily based on ultrasound, small residual or flattened multiloculated fluid collections may have been undetected, and complete radiologic resolution cannot be definitively confirmed.
Our two-session protocol showed favorable preliminary outcomes in terms of efficiency and treatment response compared to the approach reported by Jeong and Kim [
6]. Although direct comparison is limited by differences in study era, patient selection, and outcome definitions, their study achieved complete resolution in only 57.1% of cases and required an average of 3.125 sessions (up to 5) with prolonged catheterization until drainage fell below 5 mL [
6]. In contrast, our method resulted in no cysts visible on follow-up ultrasound at 6 months in all patients, while requiring only two sessions. This approach eliminates the need for extended catheterization and may simplify the treatment process while suggesting favorable efficacy. Our exclusive use of ethanol also provides a clearer evaluation of its effectiveness compared to previous studies that mixed sclerosing agents [
6].
Preservation of ovarian function is an important consideration in the management of PICs, particularly in reproductive-age women [
1]. In the present study, AMH levels were available in four patients and showed heterogeneous changes following treatment. Given the small sample size and incomplete data, these findings should be considered exploratory only, and no definitive conclusions can be drawn regarding the impact of the procedure on ovarian reserve. Therefore, these results should be interpreted with caution. Further studies with larger cohorts and systematic hormonal assessment are required to clarify this issue.
The pathogenesis of PICs is linked to the failure of the peritoneal surface to resorb physiological fluid produced by the ovaries, often due to pre-existing adhesions [
2,
3]. In our cohort, all six patients had clear etiologies involving major abdominal or pelvic surgeries. The clinical challenge is the rapid recurrence of PICs after simple aspiration. By utilizing ethanol as a sclerosing agent, we aimed to denature the mesothelial lining of the cyst wall, thereby preventing further fluid accumulation. This approach is analogous to the principle of ethanol sclerotherapy for endometriomas, which targets the destruction of the active epithelial lining to inhibit recurrence [
9]. Our results, showing a 100% technical success rate and absence of visible cysts on ultrasound at 6 months, suggest that ethanol may effectively obliterate these secreting surfaces in PICs, although larger studies are needed to confirm this mechanism.
Therapeutic efficacy was primarily assessed through changes in the maximum diameter of the cysts. While volumetric reduction may provide a more comprehensive assessment, accurate volume measurement was technically challenging. Due to the inherent nature of PICs, which lack a rigid wall and conform to the shape of adjacent pelvic organs, the cysts often became flattened rather than shrinking proportionally post-sclerotherapy. Consequently, as calculating a precise volume using standard geometric formulas was considered prone to potential error, the maximum diameter was utilized as a more reliable and reproducible metric for follow-up.
Selecting a transabdominal or transvaginal access route is crucial for procedural safety. We primarily used the transabdominal approach, opting for transvaginal access for a deeply located cyst at risk of bowel injury. High-resolution ultrasound guidance facilitated precise needle placement even in complex pelvic environments. Furthermore, using a pigtail catheter for complete drainage before ethanol instillation ensured maximal contact between the sclerosing agent and the cyst wall, which is essential for preventing recurrence [
4]. We primarily utilized 8.5-Fr pigtail catheters with multiple side holes (BSL type, Cook Medical) for efficient and thorough drainage. Compared to the standard Dawson-Mueller type, the BSL type features a greater number of side holes distributed over a larger area, which enables more effective evacuation of the cyst fluid from a wider range. However, if initial aspiration with an 8.5-Fr catheter is insufficient—as occurred in one patient in this study—we recommend upsizing to a 10.2-Fr catheter to ensure adequate drainage, which is vital to prevent ethanol dilution and ensure effective contact with the inner surface of the collapsed cyst.
Safety concerns regarding ethanol sclerotherapy include the risks of chemical peritonitis or injury to adjacent adnexal structures. In our series, we limited the maximum ethanol volume to 150 mL per session to minimize potential systemic absorption or leakage. We observed no major complications such as hemorrhage or bowel injury.
Despite its promising results, this study is limited by its small sample size and retrospective design. The small number of patients, although all demonstrated a consistent clinical response, restricted the statistical power of the findings. Additionally, follow-up imaging was primarily performed using ultrasound, which may have limited sensitivity for detecting small residual cysts or flattened multiloculated fluid collections; therefore, true complete radiologic resolution cannot be definitively confirmed. Furthermore, the follow-up duration of 6 months may be insufficient to fully assess long-term durability and recurrence. Although no recurrences were observed during this period, longer-term follow-up data, including the longest follow-up duration for each patient, were not consistently available, and delayed recurrence cannot be excluded. In addition, although the study aimed to apply a standardized protocol, a minor modification was introduced during the study period, with the maximum ethanol volume increased from 100 mL to 150 mL in the final two cases. This within-study adjustment may limit the strict uniformity of the protocol and should be considered when interpreting the results. Future prospective studies with larger cohorts and extended follow-up periods are warranted to validate these findings.
Standardized two-session catheter-directed ethanol sclerotherapy demonstrated promising short-term clinical and radiologic outcomes in this preliminary series of patients with symptomatic PICs. This minimally invasive approach may represent a feasible treatment option and potential alternative to surgery in selected patients, although larger prospective studies with long-term follow-up are required.
Conflict of interest
Gun Ha Kim, a contributing editor of the Korean Journal of Interventional Radiology, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Funding
None.
Acknowledgments
None.
Author contributions
Conceptualization: BSI, JHK, JHS. Data curation: BSI, JHK. Formal analysis: BSI, JHK, GHK, SAHA. Investigation: BSI, JHK. Methodology: BSI, JHK, GHK, SAHA. Project administration: BSI, JHK. Resources: BSI, JHK. Software: BSI, JHK. Supervision: JHS. Validation: GHK, SAHA. Visualization: BSI, JHK. Writing of the original draft: BSI, JHK. Writing of the review & editing: GHK, SAHA, JHS.
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
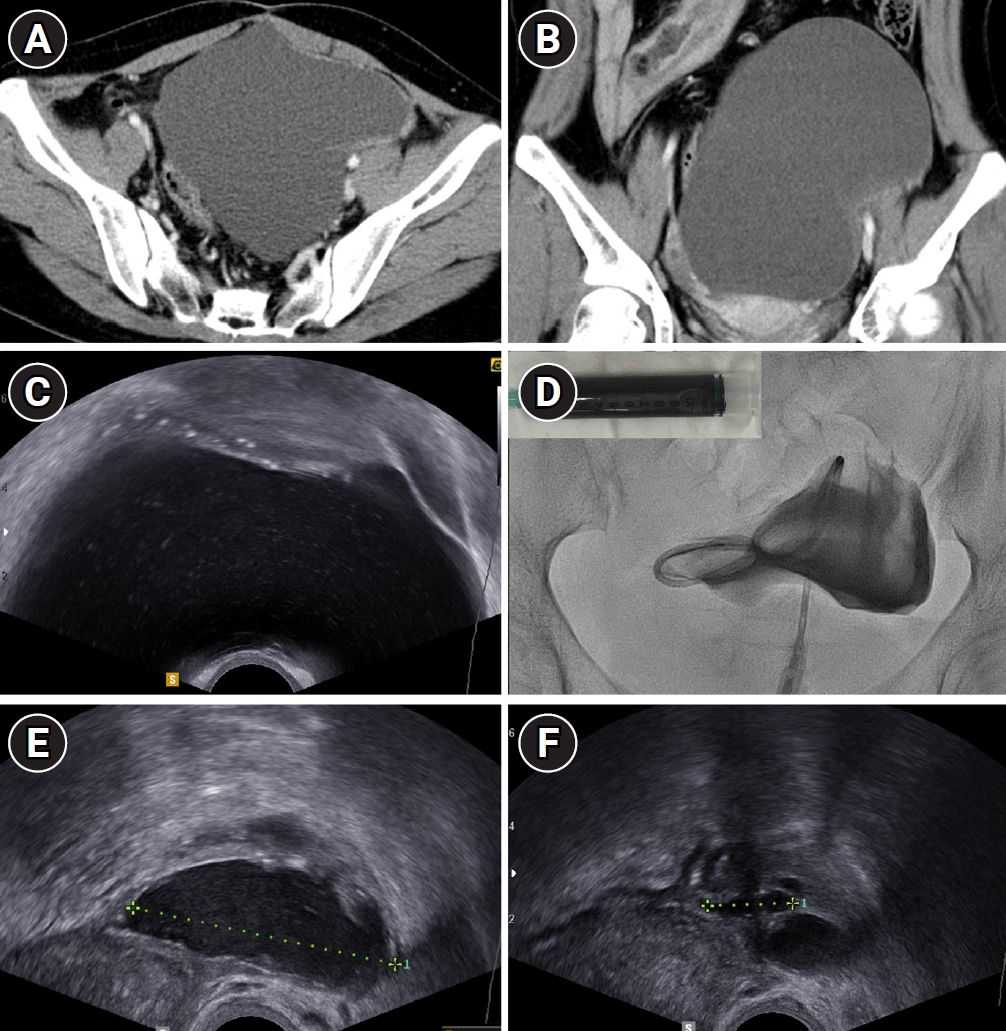
Fig. 1.A 29-year-old female with pelvic pain (case 1). Axial (A) and coronal (B) contrast-enhanced CT scans demonstrated a large cystic lesion (maximum diameter, 17.5 cm) within the pelvis. (C) Transabdominal ultrasound confirmed the presence of the large cystic lesion. (D) Following transabdominal access, an 8.5-Fr pigtail catheter with multiple side holes was inserted. A total of 1,060 mL of darkish, thin fluid was aspirated (inset), and contrast injection confirmed the absence of leakage into the peritoneal cavity. Follow-up transvaginal ultrasound images obtained 26 days (E) and 3 months (F) after two-session ethanol sclerotherapy showed a progressive reduction in cyst size with a flattened appearance; the diameters decreased to 5.5 cm and 1.8 cm, respectively. At the 6-month follow-up, the lesion was no longer visible on ultrasound (not shown).
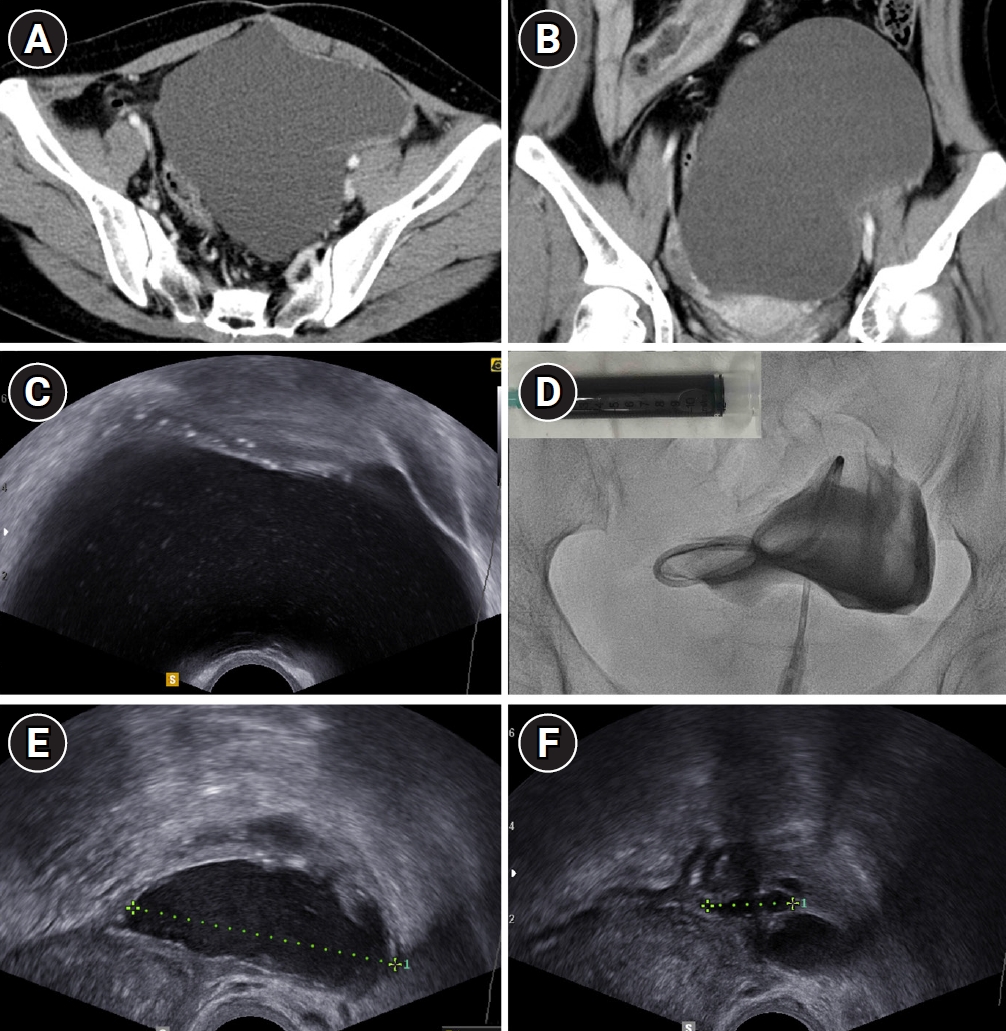
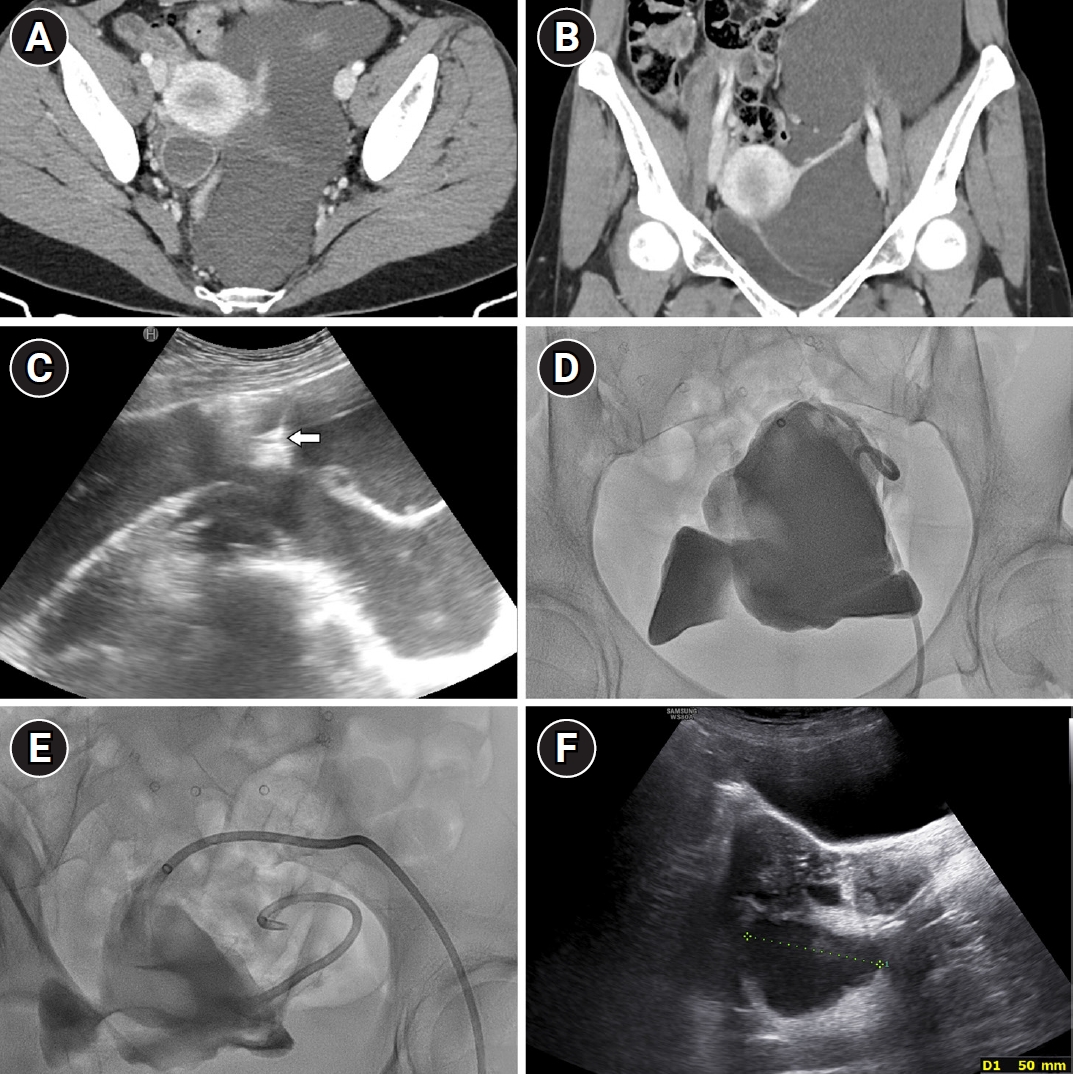
Fig. 2.A 36-year-old female with pelvic pain (case 6). Axial (A) and coronal (B) contrast-enhanced CT scans showed a 20-cm multi-lobulated pelvic cystic lesion. (C) Transabdominal ultrasound showed the initial puncture using a 21-gauge Chiba needle (arrow). (D) Tubogram showed no leakage after 1,060 mL of straw-colored fluid had been drained via an 8.5-Fr pigtail catheter, but further aspiration became difficult. (E) Following an exchange over a guidewire, a 10.2-Fr pigtail catheter was placed, allowing complete aspiration. Tubograms in (D) and (E) show the multi-lobulated nature of the cyst. (F) Follow-up transabdominal ultrasound at 19 days after two-session ethanol sclerotherapy showed a reduction in the lesion size to 5 cm. At the 3-month follow-up, the lesion was no longer visible (not shown).
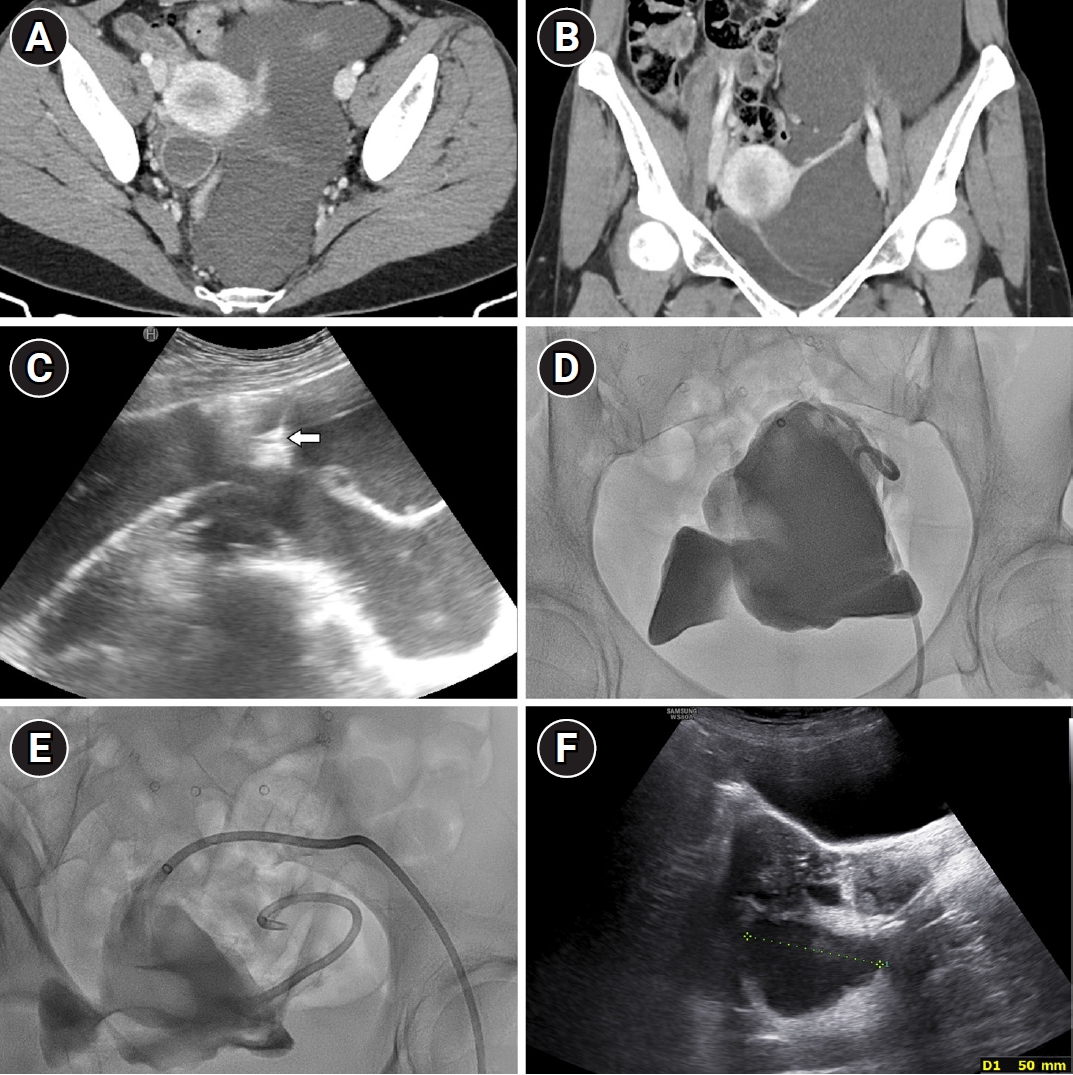
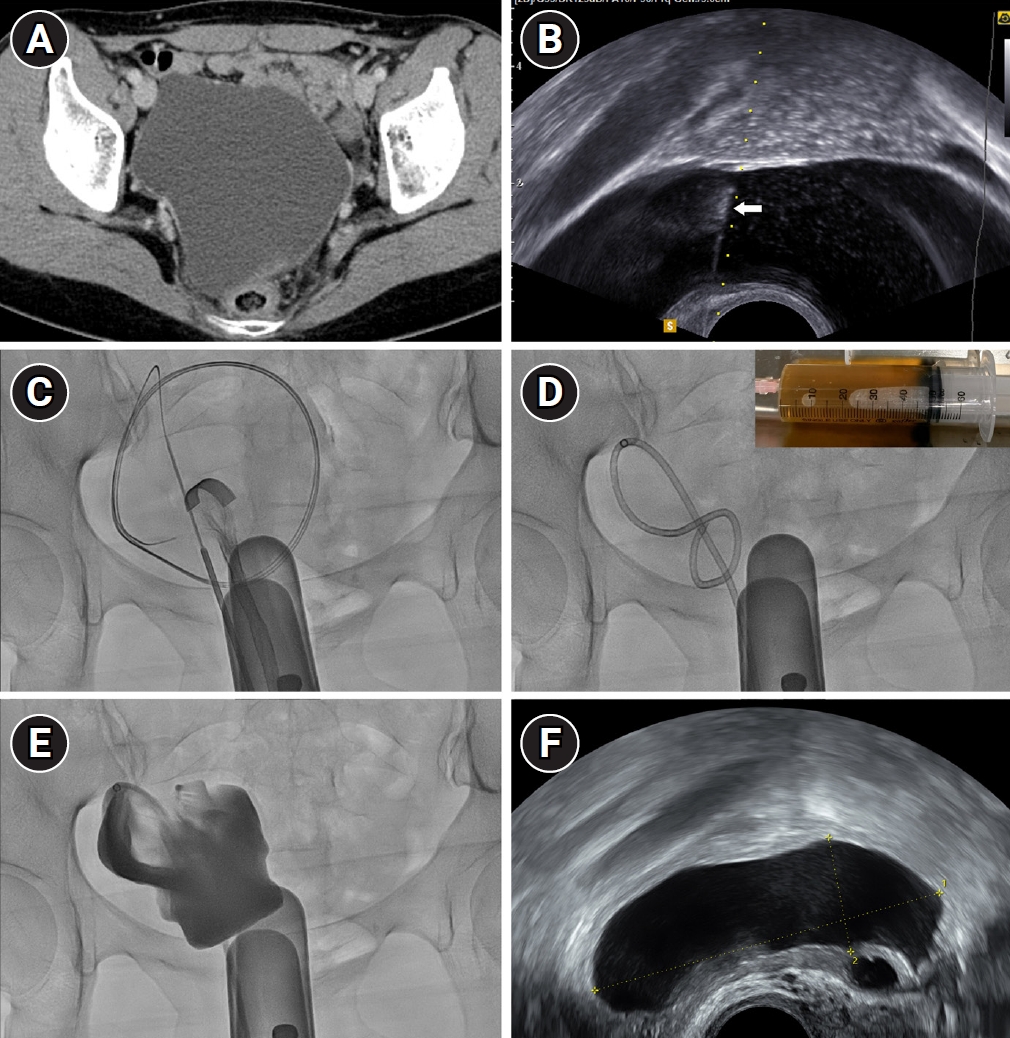
Fig. 3.A 43-year-old female with pelvic fullness (case 4). (A) Axial contrast-enhanced CT showed a 12.2-cm pelvic cystic lesion. Transabdominal access was not feasible owing to overlying bowel loops. (B) Transvaginal ultrasound demonstrated needle tract during puncture with an 18-gauge Chiba needle (arrow). (C, D) Fluoroscopic images showed guidewire insertion, which was followed by the placement of an 8.5-Fr pigtail catheter. Note the evacuated straw-colored fluid (inset in D). (E) Tubogram confirmed no contrast leakage. (F) Follow-up transvaginal ultrasound at 15 days after two-session ethanol sclerotherapy showed that the lesion decreased to 7.1 cm. At the 3-month follow-up, the lesion was no longer visible (not shown).
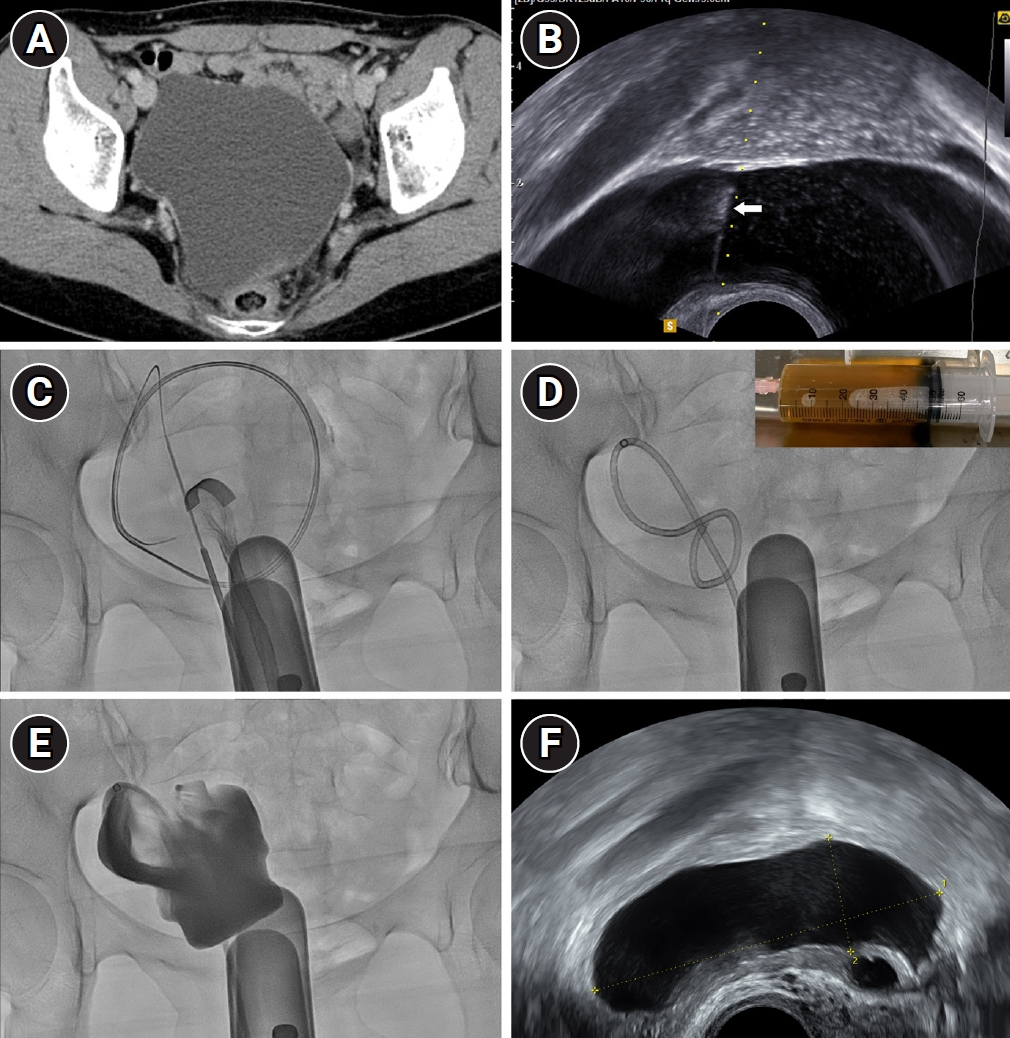
Table 1.Procedural characteristics and follow-up results of ethanol sclerotherapy
Table 1.
|
No. |
Age (years) |
Symptom |
Etiology |
Access |
Catheter |
Drainage (mL) |
Fluid nature |
Ethanol volume (mL), 1st/2nd |
Diameter (cm) |
AMH (ng/mL) |
|
Pre |
Within 1 month |
3 months |
6 months |
Prea
|
Post |
|
1 |
29 |
Pelvic pain |
Bowel resection for Crohn disease 12 YA |
TA |
8.5-Fr |
1,060 |
Darkish, thin |
100/100 |
17.5 |
5.5 (26 days) |
1.8 |
NV |
0.92 |
1.03 (3 months), 0.81 (6 months) |
|
2 |
48 |
Pelvic pain |
Hysterectomy for myoma 1.8 YA |
TA |
8.5-Fr |
910 |
Straw, thin |
100/100 |
15 |
2 (30 days) |
NV |
NV |
NA |
NA |
|
3 |
23 |
Pelvic pain |
Cloacal anomaly correction 22 YA |
TA |
8.5-Fr |
85 |
Straw, thin |
42/42 |
6 |
4 (16 days) |
NV |
NV |
NA |
3.46 (3 months) |
|
4 |
43 |
Pelvic fullness |
Cesarean section 14 YA |
TV |
8.5-Fr |
200 |
Straw, thin |
100/100 |
12.2 |
7.1 (15 days) |
NV |
NV |
0.09 |
0.28 (3 months), 0.25 (6 months) |
|
5 |
29 |
Pelvic pain |
Megacolon operation 28 YA |
TA |
8.5-Fr |
430 |
Straw, thin |
150/150 |
13 |
8 (19 days) |
NV |
NV |
2.21 |
1.47 (3 months), 1.6 (6 months) |
|
6 |
36 |
Pelvic pain |
Splenectomy and incisional hernia repair 15 YA |
TA |
10.2-Frb
|
1,060 |
Straw, thin |
150/150 |
20c
|
5.0 (19 days) |
NV |
NV |
3.14 |
2.76 (3 months) |
References
- 1. Vallerie AM, Lerner JP, Wright JD, Baxi LV. Peritoneal inclusion cysts: a review. Obstet Gynecol Surv. 2009;64:321-334. https://doi.org/10.1097/OGX.0b013e31819f93d4
- 2. Koninckx PR, Renaer M, Brosens IA. Origin of peritoneal fluid in women: an ovarian exudation product. Br J Obstet Gynaecol. 1980;87:177-183. https://doi.org/10.1111/j.1471-0528.1980.tb04514.x
- 3. Hoffer FA, Kozakewich H, Colodny A, Goldstein DP. Peritoneal inclusion cysts: ovarian fluid in peritoneal adhesions. Radiology. 1988;169:189-191. https://doi.org/10.1148/radiology.169.1.3047785
- 4. Risner V, Gonzales E, McColgan Y, Salazar G. Interventional radiology treatments to address chronic pelvic pain in females. Cardiovasc Intervent Radiol. 2025;48:950-962. https://doi.org/10.1007/s00270-024-03823-9
- 5. Ross MJ, Welch WR, Scully RE. Multilocular peritoneal inclusion cysts (so-called cystic mesotheliomas). Cancer. 1989;64:1336-1346. https://doi.org/10.1002/1097-0142(19890915)64:6<1336::aid-cncr2820640628>3.0.co;2-x
- 6. Jeong JY, Kim SH. Sclerotherapy of peritoneal inclusion cysts: preliminary results in seven patients. Korean J Radiol. 2001;2:164-170. https://doi.org/10.3348/kjr.2001.2.3.164
- 7. Lipitz S, Seidman DS, Schiff E, Achiron R, Menczer J. Treatment of pelvic peritoneal cysts by drainage and ethanol instillation. Obstet Gynecol. 1995;86:297-299. https://doi.org/10.1016/0029-7844(95)00157-m
- 8. Karakas HM, Yildirim G. Percutaneous treatment of simple renal cysts with 24-h-interval ethanol sclerotherapy. Radiol Bras. 2023;56:8-12. https://doi.org/10.1590/0100-3984.2022.0041
- 9. Zeng CH, Shin JH. Techniques and clinical outcomes of catheter-directed sclerotherapy using ethanol for ovarian endometriomas. J Korean Soc Radiol. 2025;86:e30. https://doi.org/10.3348/jksr.2025.0021
- 10. Han K, Seo SK, Kim MD, Kim GM, Kwon JH, Kim HJ, et al. Catheter-directed sclerotherapy for ovarian endometrioma: short-term outcomes. Radiology. 2018;289:854-859. https://doi.org/10.1148/radiol.2018180606
- 11. Noma J, Yoshida N. Efficacy of ethanol sclerotherapy for ovarian endometriomas. Int J Gynaecol Obstet. 2001;72:35-39. https://doi.org/10.1016/s0020-7292(00)00307-6
- 12. Omary RA, Bettmann MA, Cardella JF, Bakal CW, Schwartzberg MS, Sacks D, et al. Quality improvement guidelines for the reporting and archiving of interventional radiology procedures. J Vasc Interv Radiol. 2003;14(9 Pt 2):S293-S295. https://doi.org/10.1097/01.rvi.0000094601.83406.e1