중심단어
Hepatocellular carcinoma, radiofrequency ablation, arterioportal shunt, coil embolization
한글 초록
70세 남자 환자가 7번 간분절(S7)에 생긴 간세포암에 대한 고주파열치료술후, 추적검사에서 발견된 간세포암에 대해 경동맥화학색전술을 받기 위해 내원하였다. 입원하여 시행한 CT 와 혈관조영실에서 이전 RFA 로 인한7번 간분절 동맥과 문맥 사이의 대량의 간동문맥단락 소견이 보여 coil과 N-butyl-2-cyanoacrylate (histoacryl; B.Braun, Tuttingen, Germany)와 Lipiodol (Guerbet, Paris, France) 1:3 혼합물을 이용하여 색전술을 시행하였다.
영문 초록
A 70-year-old male patient admitted to the hospital for transarterial chemoembolization (TACE) of HCC which was found on a follow-up study after RFA of HCC in the S7. Pre-TACE dynamic CT and angiography showed massive arterioportal shunt due to the previous RFA. The patient underwent selective embolization of the shunt with coils and an N-butyl-2 cyanoacrylate (histoacryl; B.Braun) and Lipiodol (Guerbet) 1:3 mixture.
Introduction
간암의 고주파 열치료술 후 합병증으로 간동문맥단락이 발생하는 경우는 드문 것으로 알려져 있고, 간동문맥 단락이 생기는 경우 복수나 정맥류 출혈과 같은 문맥고혈압에 의한 증상이 나타날 수 있다고 알려져 있다. 이러한 간동문맥단락의 진단과 치료에는 혈관조영술이 주로 시행되고 있으며, 고주파 열치료술 후 문맥고혈압의 증상이 새로 생기거나 악화되는 경우 간동문맥단락의 의심하에 간동문맥단락의 선택적 색전술을 고려할 수 있다.
Case report
증례
70세/남자
임상소견
환자는 기저질환으로 B형 간염과 알코올성 간경변을 가진 환자로, 검진에서 발견된 7번 간분절(S7)의 간세포암에 대한 고주파 열치료술을 받은 뒤 복수가 새롭게 발생하였다. 이로 인해 환자의 Child-Pugh score는 A6에서 B7으로 악화되었다. 환자는 추적검사로 시행한 조영 전산화 단층촬영(CT) 검사에서 7번 간분절(S7)에 기존 치료부위 주위로 국소재발이 의심되어 경동맥화학색전술(TACE)가 의뢰되었고, TACE를 위해 시행한 간동맥의 선택적 조영술에서 대량의 간동문맥단락이 발견되어 치료가 계획되었다.
진단명
Massive arterioportal shunt between the S7 hepatic artery and portal vein.
영상소견
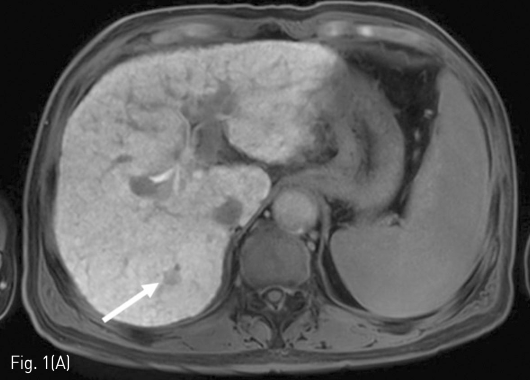
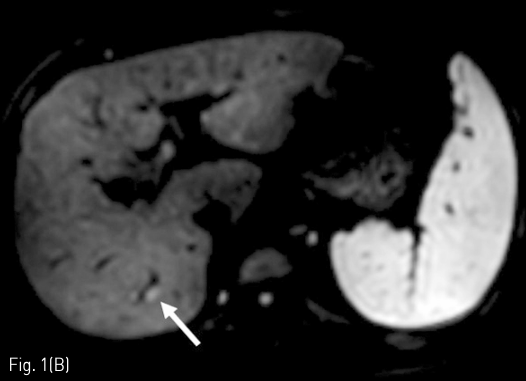
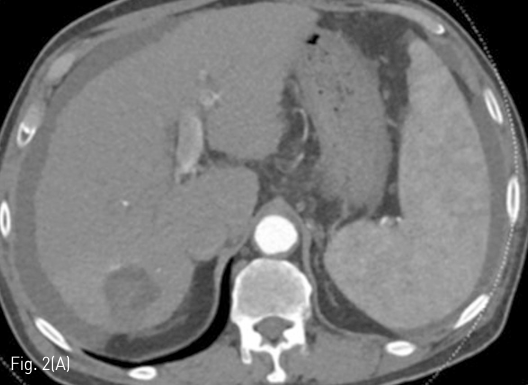
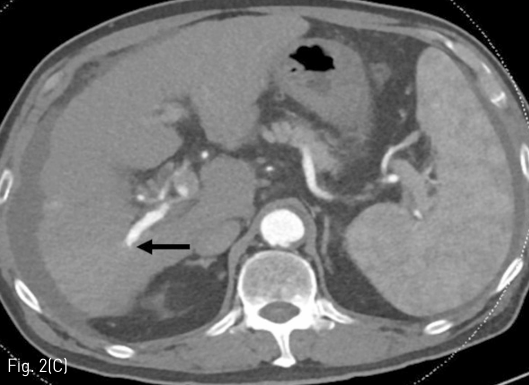
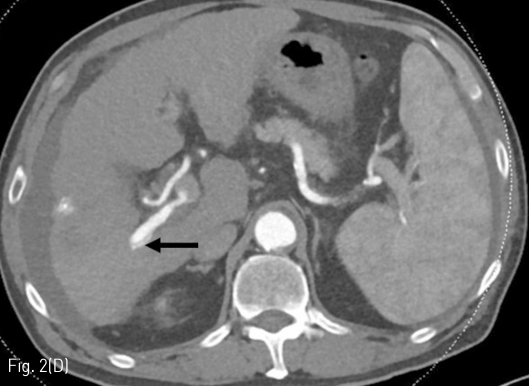
정기적 추적검사로 시행한 자기공명영상 (MRI)에서 7번 간분절(S7)에 간담도기에 저신호강도로 보이고 확산강조영상에서 고신호강도로 보이는 간암으로 의심되는 결절이 발견되어 고주파 열치료술이 시행되었다 (Fig. 1A, 1B). 10개월 후 추적검사로 시행한 전산화 단층 촬영의 동맥기 영상에서 우측 후방 간문맥이 주위 간동맥만큼 조영증강이 되는 소견을 보이고 있다(Fig. 1C, 1D). 동맥기 영상에서 간동맥과 간문맥 사이에 연결성이 보여 간동문맥단락이 의심되는 소견을 보이고 있다(Fig. 2).
시술방법 및 재료
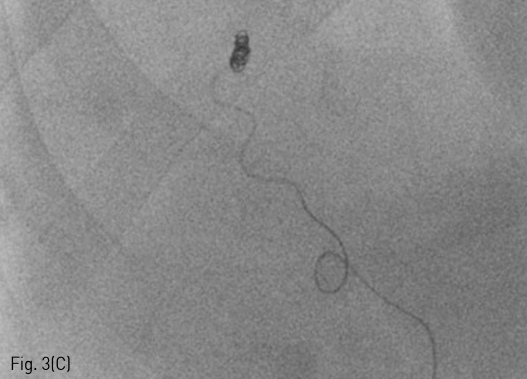
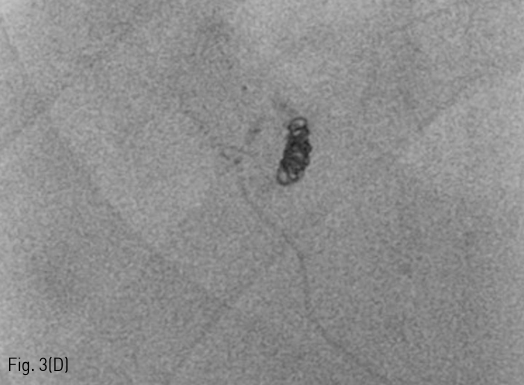
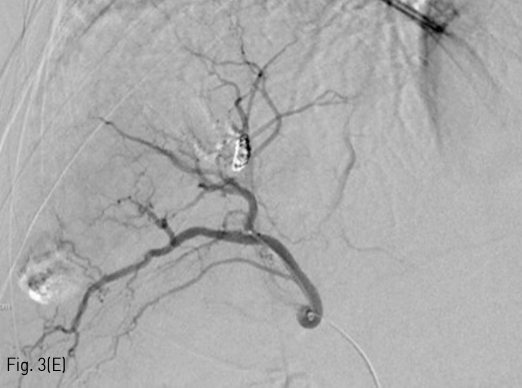
5Fr RH catheter (Cook, IN, USA)를 이용하여 총간동맥을 선택한 후 시행한 선택적 조영술에서 우측 후방 간문맥이 조영되면서 7번 간분절 동맥과 문맥 사이의 대량의 간동문맥단락 소견이 있었다(Fig. 3A, 3B). 1.9Fr microcatheter (Radiostar, Taewoong, Gyeonggi-do, Korea) 를 이용하여 간동문맥단락의 원인이 되는 혈관을 superselection 한 후, Interlock detachable coil (Boston scientific, MA, USA) 2mmx6cm과 K3 pushable coil (Taewoong, Gyeonggi-do, Korea) 2mmx2cm, 2mmx5cm을 이용하여 코일 색전술을 시행하였다 (Fig. 3C). 추가로 N-butyl-2-cyanoacrylate (histoacryl; B.Braun)와 Lipiodol (Guerbet) 1:3 혼합물 0.5mL을 이용하여 색전술을 시행하였다 (Fig. 3D). 색전술 후 시행한 간동맥의 선택적 조영술에서 간동문맥단락이 소실됨을 확인하였다(Fig. 3E).
추적관찰
환자 간동문맥단락에 대한 색전술 시행 후 복수 감소하는 소견 보였으며 이에 따라 환자의 Child-Pugh score는 B7에서 A6로 호전되었다.
Fig 1A
Massive arterioportal shunt after RFA. (A-B) A 1cm-sized tumor (arrow) was identified as low signal intensity on the hepatobiliary phase and high signal intensity on diffusion weighted imaging in the S7 of the liver.
Fig 1B
Massive arterioportal shunt after RFA. (A-B) A 1cm-sized tumor (arrow) was identified as low signal intensity on the hepatobiliary phase and high signal intensity on diffusion weighted imaging in the S7 of the liver.
Fig 1C
(C-D) RFA was conducted and follow-up liver CT was performed a month after the treatment. On an arterial phase image, the right posterior portal vein (arrow heads) showed hyperenhancement as much as the adjacent hepatic artery.
Fig 1D
(C-D) RFA was conducted and follow-up liver CT was performed a month after the treatment. On an arterial phase image, the right posterior portal vein (arrow heads) showed hyperenhancement as much as the adjacent hepatic artery.
Fig 2A
Follow up liver CT 11 months after RFA. (A-D) There is a connection (arrows) between a branch of the S7 segmental hepatic artery and right posterior portal vein.
Fig 2B
Follow up liver CT 11 months after RFA. (A-D) There is a connection (arrows) between a branch of the S7 segmental hepatic artery and right posterior portal vein.
Fig 2C
Follow up liver CT 11 months after RFA. (A-D) There is a connection (arrows) between a branch of the S7 segmental hepatic artery and right posterior portal vein.
Fig 2D
Follow up liver CT 11 months after RFA. (A-D) There is a connection (arrows) between a branch of the S7 segmental hepatic artery and right posterior portal vein.
Fig 3A
Embolization of massive arterioportal shunt. The common hepatic arteriography (A) and S7 segmental hepatic arteriography (B) showed massive arterioportal shunt (arrowhead) between a branch of the S7 segmental hepatic artery and right posterior portal vein. A connection (arrow) between the S7 segmental hepatic artery and right posterior portal vein was identified on arteriography.
Fig 3C
(C) The shunt was embolized with detachable and pushable coils.
Fig 3D
(D) Additional embolization was performed with a mixture of Lipiodol and NBCA (volume ratio, 3:1).
Fig 3E
(E) Post-embolization arteriography showed complete occlusion of arterioportal shunt.
고찰
간암의 고주파 열치료술은 간암에 대한 치료로 흔히 시행되는 시술로, 여러 연구에서 우수한 치료성적이 입증되어 최근 많이 행해지고 있다. 시술에 따른 합병증으로 수술이나 색전술이 필요한 복강내출혈, 간농양, 소화기관 천공 등 주요한 합병증부터 간동문맥단락, 담도문맥단락, 간 피막하출혈 등 비교적 경미한 합병증까지 다양한 증례가 보고되고 있다. 그 중에서 간동문맥단락은 드문 합병증으로 알려져 있고, 그 크기나 단락의 양이 작을 경우 무증상인 경우가 많다고 알려져 있다. 그러나 단락의 크기가 크고 양이 많은 경우 복수나 정맥류 등 문맥압항진에 의한 증상이 새로 생기거나 악화될 수 있어 치료를 필요로 하게 된다. 간동문맥단락의 치료의 경우 혈관조영술을 통한 검사와 치료가 주로 시행되고 있다. 따라서 간암의 고주파 열치료술 후 복수나 정맥류 등 문맥압항진에 의한 증상이 새로 생기거나 기존의 증상이 악화되는 경우 선택적색전술을 고려할 필요가 있다. 간동문맥단락의 정확한 위치와 크기를 혈관조영술 상에서 정확히 알기가 어려운 경우가 있는데, 이 때는 C-arm CT 영상을 얻는 것이 도움이 된다. 이번 증례와 같이 단락의 크기가 크고 양이 많은 경우 빠른 혈류로 인해 문맥쪽으로 색전물질이 씻겨 나갈 위험이 있으므로, 코일을 이용하여 단락의 양을 줄인 뒤에 N-butyl 2-cyanoacrylate 를 사용하는 것이 도움이 된다. 기존의 한 보고에서는 전산화 단층 촬영의 용적 재현 영상(volume-rendered image)를 이용하여 간동문맥단락의 정확한 위치와 크기를 진단할 수 있었고, 풍선카테터를 고유간동맥에 넣어 간동문맥단락으로의 빠른 혈류를 차단한 후 N-butyl-2-cyanoacrylate 와 Lipiodol (Guerbet) 혼합물을 이용하여 색전술을 성공적으로 시행하였다. 이번 증례에서도 간동문맥단락의 정확한 위치를 진단하는데 전산화 단층 영상이 사용되었고, 코일색전술을 통해 간동문맥단락으로의 혈류를 느리게 한 뒤에 N-butyl-2-cyanoacrylate (histoacryl; B.Braun)와 Lipiodol (Guerbet) 혼합물을 사용하여 성공적으로색전술을 시행하였다.
참고문헌
1. Livraghi T, Solbiati L, Meloni MF, Gazelle GS, Halpern EF, Goldberg SN. Treatment of focal liver tumors with percutaneous radio-frequency ablation: complications encountered in a multicenter study. Radiology 2003;226:441-451
2. Sonomura T, Kawai N, Kishi K, et al. N-butyl cyanoacrylate embolization with blood flow control of an arterioportal shunt that developed after radiofrequency ablation of hepatocellular carcinoma. Korean J Radiol 2014;15:250-253
3. Kanogawa N, Chiba T, Ogasawara S, et al. Successful interventional treatment for arterioportal fistula caused by radiofrequency ablation for hepatocellular carcinoma. Case Rep Oncol 2014;7:833-839
4. Chen Q, Tack C, Morcos M, et al. Embolotherapy of an arterioportal fistula. Cardiovasc intervent Radiol 2007;30:1047-1051
5. Lazaridis KN, Kamath PS. Images in hepatology. Arterio-portal fistula causing recurrent variceal bleeding. J Hepatol 1998;29:142
Citations
Citations to this article as recorded by