중심단어
Partial nephrectomy, urinary leakage, urinoma, percutaneous embolization
한글 초록
부분 신장절 제술 후 요누출은 비교적 잘 알려진 수술 후 발생 가능한 합병증으로, 부분 신장 절제술을 시행 받은 환자의 0.78%~17.4%의 빈도로 보고되고 있다. 부분 신장 절제술 후 발생한 요누출은 대개의 경우 보전적 치료로 호전되는 경우가 많으나, 지속적인 요누출의 경우 적극적인 치료가 필요하다. 본 증례에서는 46세 여자 환자가 우측 신장에 종양이 발견되어 우측 신장 부분 절제술을 시행 받았고, 수술 후 5일째에 발생한 우측 상복부 통증에 대해 전산화 단층촬영에서 요누출로 인한 요종이 확인되었다. 요누출에 대해서 경피적 색전술을 통하여 성공적으로 치료할 수 있었다.
영문 초록
Urinary leakage after partial nephrectomy is a well-described complication in previous literatures, which was reported in 0.78% to 17.4% of patients underwent for partial nephrectomy. Although it is usually resolved with proper conservative management, urinary leakage complications following partial nephrectomy may persist. Therefore, other management modalities are indicated such as percutaneous drainage, nephrostomy, and ureteral stent placement. However, if failed rarely surgical correction to repair the urinary fistula or even radical nephrectomy is needed. Meanwhile, successful using of adhesive materials such as fibrin or N-Butyl cyanoacrylate was previously reported in literatures to avoid risks associated with second surgical interventional or radical nephrectomy. Adhesive materials were injected along the leakage tract to seal orifice of the fistula and to prevent formation of urinoma. In this case report, we present a case of urinary leakage after partial nephrectomy which was successfully treated by percutaneous embolization.
Introduction
부분 신장 절제술 후 발생한 요누출은 대개의 경우 보전적 치료로 호전되는 경우가 많으나, 지속적인 요누출의 경우 적극적인 치료가 필요하다. 경피적 배액 솔, 신루설치술, 요관 스텐트 삽입술 등을 통해 요누출을 치료할 수 있으며, 본 증례에서는 부분 신장 절제술 후에 발생한 요누출에 대해서 경피적 색전술 치료법에 대해서 보고하고자 한다.
Case report
증례
46세/여자
임상소견
유방암으로 수술 및 항암치료를 받은 과거력이 있는 환자로, 정기 추적관찰에서 우측 신장에 종양이 발견되어 우측 신장 부분 절제술을 시행 받았고, 수술 후 5일째 우측 상복부 통증을 호소함.
진단명
Urinary leakage after partial nephrectomy
영상소견
조영 증강 복부 전산화 단층촬영에서 우측 신장에 renal cell carcinoma로 생각되는 약 3cm 크기의 hypervascular tumor가 있다 (Fig. 1A) 우측 신장 부분 절제술을 시행 받고 5일째 복통을 호소하여 시행한 복부 전산화 단층촬영에서 수술 부위 주변으로 large urinoma with contrast leakage를 확인할 수 있다 (Fig. 1B).
시술방법 및 재료
우측 신장 부분 절제술 주변 large urinoma에 대해서 경피적 배액술을 먼저 시행하기로 계획하였고, 이에 Rt. lateral abdominal wall을 국소 마취한 후 right partial nephrectomy site 주변부 urinoma를 21G needle (Tae Chang Industrial, Taegu, Korea)로 천 자 하고, 8.5Fr pigtail catheter (Cook, Bloomington, IN)를 삽입하여 urinoma 배액술을 시행하였다 (Fig. 2A). 배액술 이후 경과 관찰하였을 때, 배액관을 통해서 160cc/day의 요누출이 지속되어 배액술 시행 12일째 urinary leakage에 대해서 embolization을 시행하기로 하였다. 배액술을 통해 cavity size 가 감소한 urinoma를 초음파 유도 하에 21G needle로 천자하고, 5Fr Kumpe catheter와 2.0Fr microcatheter (Progreat, Terumo, Tokyo, Japan)을 이용하여 partial nephrectomy site로부터 urinoma로의 fistulous tract을 찾는데 성공하였고 (Fig. 2B), 조영제를 주입하였을 때 뚜렷한 fistulous tract이 존재함을 확인하였다 (Fig. 2C). 이후 해당 fistulous tract을 MicroNester coil (3mmx2cmx6ea, Cook)을 이용하여 embolization 시행하였고, urinoma cavity를 N-Butyl cyanoacrylate (Histoacryl, B. Braun, Rubi, Spain) 2 vial 과 iodized oil (Lipiodol Ultra Fluide; Guerbet, Roissy, France) 1:1 mixture를 사용하여 obliteration 하고 pigtail catheter는 제거하였다 (Fig. 2D). 시술 직후 시행한 초음파에서 residual urinoma cavity는 관찰되지 않았다.
추적관찰
경피적 색전술 후 환자 증상 호전되었으며, 약 15개 월 후 외래 경과 관찰하면서 시행한 조영증강 복부 전산화 단층촬영에서 urinoma는 소실되었고 fistulous tract은 coil에 의해 compact occlusion되어있음을 확인하였다(Fig. 3).
Fig 1A
(A) A 46-year-old female underwent partial nephrectomy for hypervascular mass (arrow) in right kidney.
Fig 1B
(B) On 5 days after the surgery, follow-up contrast enhanced CT shows large urinoma with contrast leakage (arrow) around the right partial nephrectomy site.
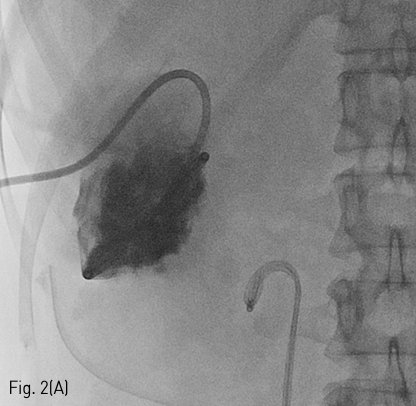
Fig 2A
(A) Spot radiograph shows percutaneous drainage catheter in the urinoma cavity.
Fig 2B
(B) Spot radiograph shows successful catheterization for urinary fistula through percutaneous access via urinoma cavity.
Fig 2C
(C) Fistulography obtained after successful catheterization for urinary fistula shows direct connection (arrow) between the renal calyx and urinoma cavity.
Fig 2D
(D) Spot radiograph obtained after successful embolization procedure shows complete occlusion of urinary fistulous tract by multiple coils (arrow) and obliteration of urinoma cavity (star) by glue cast.
Fig 3
Regular follow-up contrast enhanced CT in 15 months later demonstrates the compact occlusion of the urinary fistulous tract by coils (arrow) without recurred urinoma.
고찰
Partial nephrectomy 이후 발생하는 urinary leakage or urinoma는 대개의 경우 보존적 치료를 통해 자연적으로 치유되는 경우가 많으며, urinoma가 지속되는 경우 배액술을 필요로 한다. 배액술 이후에 urinoma의 크기가 감소하지 않거나, 배액량이 감소하지 않을 경우에는 partial nephrectomy site로부터의 fistula의 가능성을 반드시 고려해보아야 한다. Fistula formation이 의심이 되면, percutaneous nephrostomy를 시행하여 urinary leakage의 healing을 기대해 보거나 urinary stenting을 통한 추가적인 urine diversion을 시도해 볼 수 있다. 그러나 배액술과 urinary diversion을 통한 치료는 urinary leakage가 치유되기까지 비교적 오랜 시간이 필요하며, 문헌 보고에 따르면 평균 53.2일의 치유 기간이 소요되었다.
최근에는 urinary fistula formation으로 인해 urinary leakage가 지속되는 환자에 대해서 minimally invasive & early intervention treatment로 fistula tract을 찾아서 adhesive fibrin or embolic material을 사용하여 occlusion 하는 치료 방법들이 보고되고 있다. Urinoma에 대한 배액술을 시행하고, 이후 antegrade or retrograde pyelograhy를 시행하여 urinary fistula formation 여부를 확인한다. Fistula formation이 명확하게 확인된다면, 해당 fistula tract을 coil 혹은 N-Butyl cyanoacrylate와 같은 embolic material을 사용하여 occlusion 하고 배액관은 즉시 제거하거나 유지하면서 배액량이 감소하면 제거할 수 있게 된다. 본 증례에서는 urinoma에 대해 경피적 배액술을 시행하였고, 이후 urinoma cavity로부터 partial nephrectomy site의 fistula tract을 찾는데 성공하였고 해당 fistula tract을 coil을 사용하여 막고 urinoma cavity를 N Butyl-cyanoacrylate를 사용하여 closure 하여 치료할 수 있었다. 이처럼 Percutaneous embolization은 partial nephrectomy 후 발생한 urinary leakage를 안전하고, 효과적이고, 빠르게 치료할 수 있는 방법임을 숙지하고 임상적으로 적용하는 것이 필요하다.
참고문헌
1. Selli C, De Maria M, Manica M, Turri FM, Manassero F. Minimally invasive treatment of urinary fistulas using Nbutyl-2-cyanoacrylate: a valid first line option. BMC Urol 2013 24;13:55
2. Aslan G, Men S, Gulcu A, Kefi A, Esen A. Percutaneous embolization of persistent urinary fistula after partial nephrectomy using N-butyl-2cyanoacrylate. Int J Urol 2005;12:838-841
3. Tekin MI, Peskircioglu L, Boyvat F, Ozkardes H. Practical approach to terminate urinary extravasation: percutaneous fistula tract embolization with N-butyl cyanoacrylate in a case with partial nephrectomy. Tech Urol 2001;7:67-69
4. Okada T, Kono Y, Matsumoto K, Utsunomiya N, Tsunemori H, Kawakita M. [Percutaneous Fibrin Glue Injection for Persistent Urinary Leakage after Partial Nephrectomy : A Case Report]. Hinyokika Kiyo. 2017;63:107-110
5. Seo IY, Lee YH, Rim JS. Case report: percutaneous fibrin glue injection for urine leakage in laparoscopic partial nephrectomy. J Endourol 2008;22:959-62
6. Muto G, D'Urso L, Castelli E, Formiconi A, Bardari F. Cyanoacrylic glue: a minimally invasive nonsurgical first line approach for the treatment of some urinary fistulas. J Urol. 2005;174:2239-2243
Citations
Citations to this article as recorded by